## Clinical Diagnosis This patient has **iron deficiency anemia (IDA)** confirmed by: - Microcytic hypochromic indices (MCV 62 fL, MCH 18 pg) - Low serum iron (32 μg/dL), low ferritin (8 ng/mL), elevated TIBC (420 μg/dL) - Low transferrin saturation (7.6%) - Peripheral smear: microcytic hypochromic RBCs with target cells - Reticulocyte count appropriately low (0.8%) — bone marrow is iron-limited ## Why GI Workup Is the Next Step **Key Point:** Although menorrhagia is an identified source of blood loss, **upper and lower GI endoscopy is recommended to exclude concurrent GI pathology** because: 1. IDA in any adult warrants investigation for all potential sources of blood loss 2. Concurrent GI pathology (peptic ulcer, celiac disease, angiodysplasia, colorectal malignancy) may coexist with menorrhagia 3. Failure to investigate GI sources can delay diagnosis of serious underlying disease, including malignancy **High-Yield (Harrison 21e, Ch 97):** The standard approach to IDA workup: - Confirm iron deficiency (ferritin, iron, TIBC, transferrin saturation) ✓ Done - Identify the source of blood loss: - In **women of reproductive age with menorrhagia**: GI endoscopy is recommended when anemia is severe (Hb <8 g/dL), recurrent, or refractory to iron supplementation — to exclude concurrent GI pathology - In **men and postmenopausal women**: GI endoscopy is mandatory **Clinical Pearl:** Severe menorrhagia can indeed cause Hb as low as 7.2 g/dL; however, current guidelines recommend GI endoscopy to exclude concurrent pathology rather than attributing all blood loss to menorrhagia alone. This is especially important in a rural setting where access to follow-up may be limited. ## Why Other Options Are Incorrect | Option | Rationale | |--------|-----------| | **Bone marrow aspiration (A)** | Not needed; serum ferritin and iron indices have already confirmed iron deficiency. Bone marrow iron stain adds no new diagnostic information beyond these markers. | | **B12 and folate levels (B)** | MCV is low (microcytic), not elevated (macrocytic). B12/folate deficiency causes macrocytic anemia; these tests are not indicated here. | | **Hemoglobin electrophoresis (D)** | Thalassemia trait is excluded by the markedly low ferritin (8 ng/mL) and low serum iron — thalassemia trait presents with normal or elevated ferritin and normal iron stores. While the RBC count of 5.8 × 10¹²/L is borderline elevated (a feature sometimes seen in thalassemia trait), the iron deficiency indices are unequivocal. Hemoglobin electrophoresis may be considered *after* iron repletion if microcytosis persists, but it is not the immediate next step. | [cite:Harrison 21e Ch 97; Hoffbrand's Essential Haematology 7e] 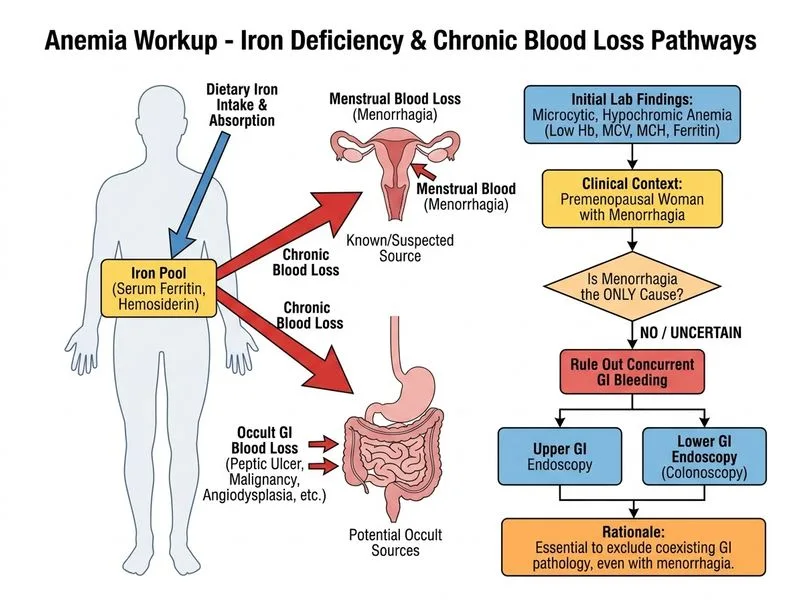
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.