## Clinical Presentation Analysis This patient has **megaloblastic anemia with concurrent folate deficiency**, as evidenced by: - Macrocytic anemia (MCV 118 fL, MCH 38 pg) - Hypersegmented neutrophils and occasional megaloblasts on smear - **Low serum B12 AND low serum folate** (both are abnormal) - Pancytopenia (Hb 6.8, WBC 2.8, platelets 95) - Neurological signs (glossitis, diminished vibration sense, positive Romberg) — consistent with B12 deficiency ## Why Concurrent Folate Deficiency? **Key Point:** Although the patient has known pernicious anemia (B12 deficiency), the **acute decompensation is precipitated by concurrent folate deficiency**. Here's why: 1. **Folate is depleted faster than B12** in the setting of megaloblastic anemia because: - Rapidly dividing cells (bone marrow, GI epithelium) consume folate stores quickly - B12 stores in the liver last years; folate stores last only months 2. **Vegetarian diet is a risk factor** for both B12 (no animal products) and folate (limited if diet lacks leafy greens, legumes) 3. **Dual deficiency causes severe pancytopenia** (WBC 2.8, platelets 95) — folate deficiency worsens bone marrow suppression 4. **Elevated LDH (680) and indirect hyperbilirubinemia (2.4)** indicate **ineffective erythropoiesis** (intramedullary hemolysis), which is characteristic of megaloblastic anemia but worsened by dual deficiency **High-Yield:** The combination of: - Known B12 deficiency (pernicious anemia) - Neurological signs (B12-specific) - **Both low B12 AND low folate on labs** - Severe pancytopenia - Elevated LDH + indirect hyperbilirubinemia → **Diagnosis: Megaloblastic anemia with concurrent folate deficiency** ## Differential Reasoning | Finding | B12 Deficiency Alone | B12 + Folate Deficiency | Hemolytic Anemia | Leukemic Transformation | |---------|----------------------|-------------------------|------------------|------------------------| | **MCV** | Elevated | Elevated | Normal/low | Variable | | **Reticulocyte count** | Low-normal (1.2%) | Low-normal | **High (>5%)** | Low | | **LDH** | Elevated (ineffective erythropoiesis) | Elevated | **Very high** | Normal/elevated | | **Indirect bilirubin** | Mild elevation | Mild elevation | **High (>3 mg/dL)** | Normal | | **Haptoglobin** | Normal | Normal | **Low** | Normal | | **Folate level** | Normal | **Low** | Normal | Normal | | **Neurological signs** | **Present** | **Present** | Absent | Absent | **Clinical Pearl:** The reticulocyte count is **inappropriately low (1.2%)** for the degree of anemia (Hb 6.8). In hemolytic anemia, reticulocyte count would be >5–10%. This rules out acute hemolysis. **Mnemonic: FOLATE TRAP** — **F**olate stores deplete **F**ast; **O**ld B12 stores last **O**ver years; **L**ow folate worsens **L**ow marrow output; **A**cute decompensation from **A**dded folate loss; **T**wo deficiencies cause **T**rue pancytopenia; **E**levated LDH from **E**ffective marrow suppression [cite:Harrison 21e Ch 98; Robbins 10e Ch 14] 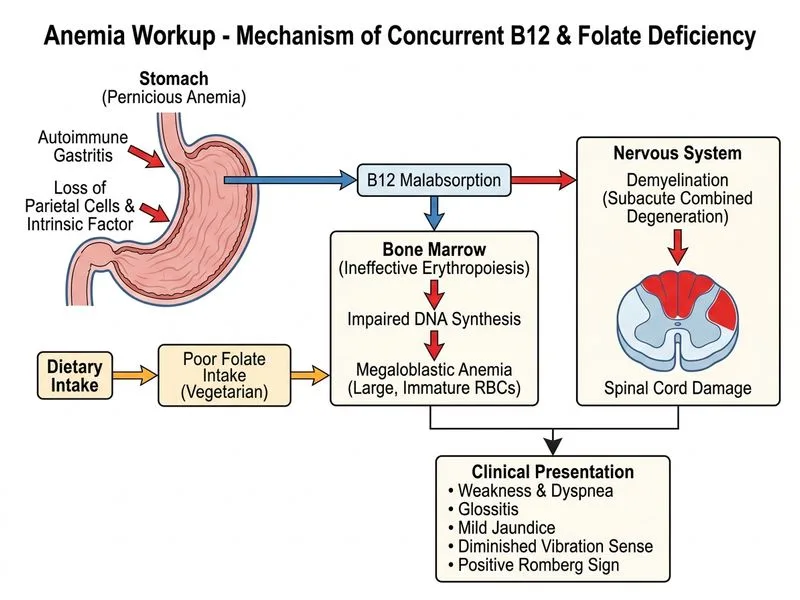
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.