## Clinical Diagnosis This patient has **iron deficiency anemia (IDA)** secondary to menorrhagia, confirmed by the classic microcytic-hypochromic pattern and depleted iron stores. ### Key Diagnostic Features **Key Point:** The constellation of microcytic anemia (MCV 62 fL), hypochromia (MCH 18 pg), elevated RBC count (5.8 million/µL — relative polycythemia), and markedly depleted iron stores (ferritin 8 ng/mL, transferrin saturation 8%) is pathognomonic for iron deficiency. **High-Yield:** The **TIBC is elevated (420 µg/dL; normal 250–425)** and **transferrin saturation is low (8%; normal 20–50%)** — this is the hallmark of iron deficiency: the body upregulates iron transport machinery in response to depletion. ### Why Oral Iron Is the Next Step **Clinical Pearl:** Once iron deficiency is confirmed biochemically and the source of blood loss is identified (menorrhagia in this case), **empiric oral iron replacement is the standard first-line therapy** — bone marrow examination is unnecessary and delays treatment. **Mnemonic: IRON REPLACEMENT CRITERIA — IDEF** - **I**dentified source of blood loss (menorrhagia ✓) - **D**epleted iron stores confirmed (ferritin, TIBC, saturation ✓) - **E**xclude other causes of anemia (B12/folate not indicated here; hemolysis ruled out by normal bilirubin context) - **F**irst-line: oral iron (ferrous sulfate 200 mg elemental iron daily) ### Dosing and Monitoring | Parameter | Details | |-----------|----------| | **First-line agent** | Ferrous sulfate 200 mg elemental iron once daily with vitamin C (enhances absorption) | | **Expected Hb rise** | 1–2 g/dL per month if adherent | | **Duration of therapy** | Continue 3–6 months after Hb normalizes to replete bone marrow stores | | **Reassess** | Repeat CBC at 4–6 weeks; if no rise, assess compliance and GI absorption | **Warning:** Do NOT order bone marrow biopsy for uncomplicated IDA — it is invasive, expensive, and unnecessary once biochemical confirmation is obtained. Reserve marrow examination for atypical presentations (e.g., concurrent cytopenias, suspected malignancy, or refractory anemia). [cite:Harrison 21e Ch 99] 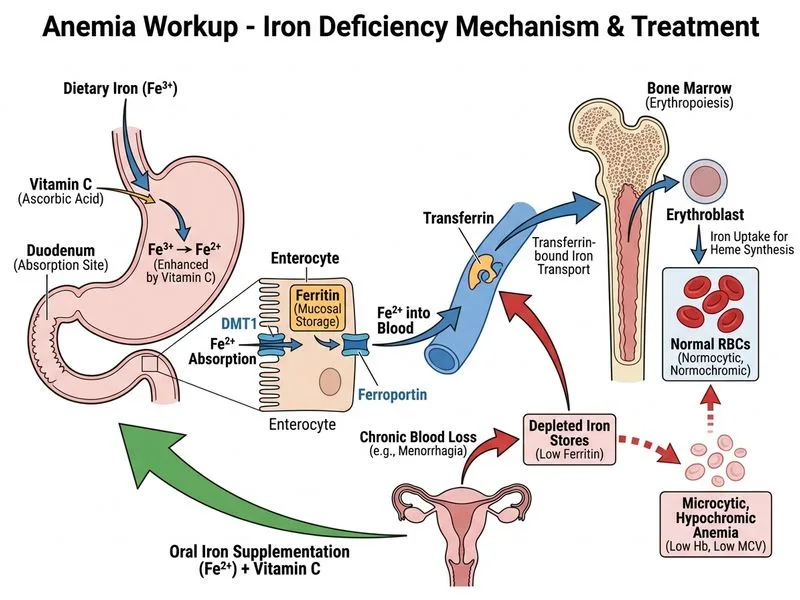
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.