## Clinical Diagnosis This patient has **anemia of chronic kidney disease (CKD)**, a normocytic normochromic anemia caused by **erythropoietin (EPO) deficiency and uremia-induced RBC survival shortening**. ### Key Diagnostic Features **Key Point:** The combination of: - **Normocytic, normochromic anemia** (MCV 88 fL, MCH 28 pg — normal indices) - **Low reticulocyte count (0.8%)** — inappropriately low for the degree of anemia; in a healthy person with Hb 8.5 g/dL, reticulocyte count should be >2–3% (indicating bone marrow response) - **Advanced CKD (eGFR 28)** with elevated creatinine and BUN - **Normal iron, B12, and folate stores** — rules out nutritional causes ...is diagnostic of **anemia of CKD from EPO deficiency**. ### Pathophysiology **High-Yield:** The kidneys produce ~90% of circulating EPO. When eGFR falls below 45 mL/min/1.73 m², EPO production declines disproportionately, leading to: 1. Decreased RBC production (low reticulocyte response) 2. Shortened RBC lifespan (uremic toxins damage RBC membrane) 3. Normocytic anemia that worsens as renal function declines **Mnemonic: ANEMIA OF CKD — CHRONIC** - **C**hronic kidney disease (eGFR <45) - **H**emoglobin typically 7–10 g/dL - **R**eticulocyte count inappropriately LOW (not elevated) - **O**rgan (kidney) fails to produce EPO - **N**ormocytic, normochromic indices - **I**ron, B12, folate are NORMAL - **C**ause: EPO deficiency + uremic RBC survival shortening ### Why Iron, B12, and Folate Are Normal | Parameter | Finding | Interpretation | |-----------|---------|----------------| | **Serum iron** | 95 µg/dL (normal 60–170) | Normal; rules out iron deficiency | | **Ferritin** | 185 ng/mL (normal 30–300) | Normal; adequate iron stores | | **TIBC** | 280 µg/dL (normal 250–425) | Normal; no upregulation of iron transport | | **Transferrin saturation** | 34% (normal 20–50%) | Normal; adequate iron availability | | **B12** | 420 pg/mL (normal >200) | Normal; no B12 deficiency | | **Folate** | 6.2 ng/mL (normal >5.4) | Normal; no folate deficiency | **Clinical Pearl:** In CKD, iron studies are typically normal or elevated (due to reduced erythropoiesis and iron recycling). Ferritin may be falsely elevated as an acute-phase reactant in chronic inflammation. ### Management **High-Yield:** First-line therapy is **erythropoietin-stimulating agents (ESAs)** such as: - Epoetin alfa or darbepoetin alfa (IV or SC) - Target Hb: 10–11 g/dL (avoid >12 g/dL due to thrombotic risk) - Iron supplementation (IV preferred in dialysis patients) to support EPO response [cite:Harrison 21e Ch 279; KDIGO 2021 Anemia in CKD Clinical Practice Guideline] 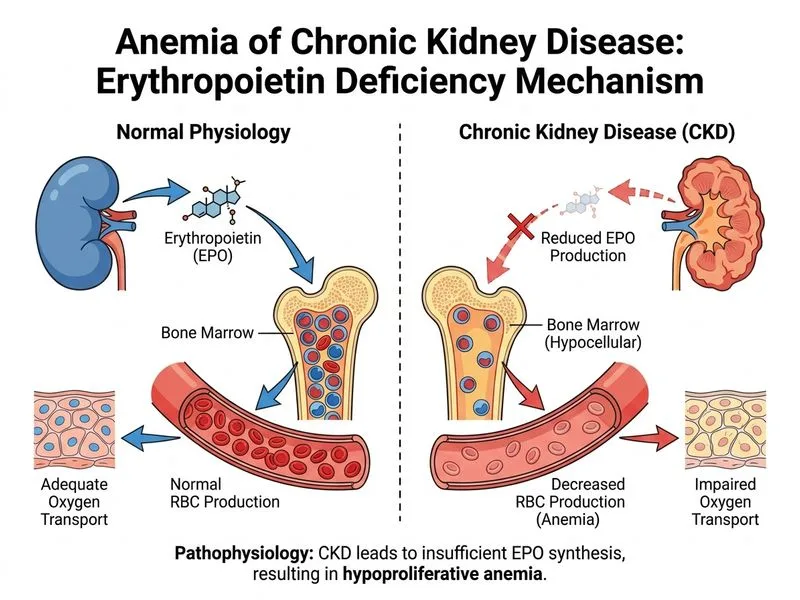
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.