Anemias Overview MCQ — NEET PG Practice Question | NEETPGAI
Anemias Overview
medium
microscope Pathology
A 28-year-old man from Delhi presents with acute-onset pallor, jaundice, and dark urine for 2 days. On examination, he is febrile (38.5°C), tachycardic, and has hepatosplenomegaly. Laboratory findings: Hb 8.9 g/dL, reticulocyte count 12%, indirect bilirubin 4.2 mg/dL, LDH 1200 IU/L, haptoglobin <10 mg/dL. Peripheral smear shows spherocytes and polychromasia. What is the most appropriate next step?
A. Perform direct antiglobulin test (DAT/Coombs test) immediately
B. Start empirical broad-spectrum antibiotics and supportive care
C. Perform urgent splenectomy
D. Initiate corticosteroid therapy 1 mg/kg prednisolone daily
Explanation
Clinical Diagnosis
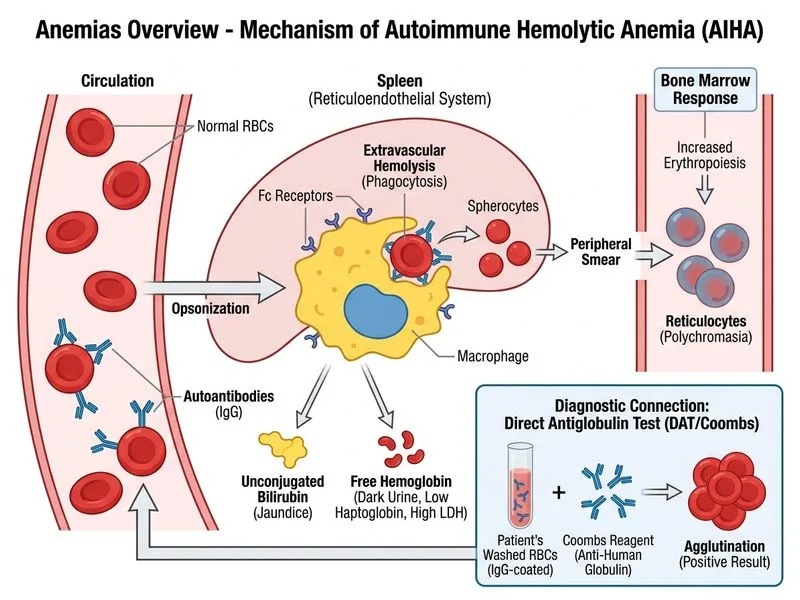
The patient presents with acute hemolytic anemia: jaundice, dark urine (hemoglobinuria), fever, spherocytes on smear, elevated reticulocyte count (12%), elevated indirect bilirubin, elevated LDH, and low haptoglobin. This constellation is pathognomonic for hemolysis.
Differential Diagnosis of Hemolytic Anemia
Key Point
The clinical presentation suggests immune-mediated hemolysis (fever, acute onset, spherocytes). The next step is to confirm the immune mechanism via the Direct Antiglobulin Test (DAT), which detects IgG/IgM and complement (C3) bound to red cell surface.
Diagnostic Algorithm
Loading diagram...
High-YieldNEET PG
DAT is the single most important confirmatory test for immune hemolytic anemia. Positive DAT + clinical hemolysis = autoimmune hemolytic anemia (AIHA). Negative DAT in hemolysis suggests non-immune causes (G6PD deficiency, hereditary spherocytosis, microangiopathic hemolytic anemia).
Why DAT First
Table
Test
Purpose
Interpretation
DAT (Coombs)
Detects IgG/IgM/C3 on RBC surface
Positive = immune-mediated hemolysis
Reticulocyte count
Assesses bone marrow response
Elevated = hemolysis or blood loss
Haptoglobin
Binds free hemoglobin
Low = active hemolysis
LDH
Released from lysed RBCs
Elevated = hemolysis
Indirect bilirubin
Heme breakdown product
Elevated = hemolysis
Clinical Pearl
Fever + acute hemolysis + positive DAT may indicate secondary AIHA (infection, lymphoma, SLE, drug-induced). However, the immediate diagnostic step is still DAT confirmation, not empirical antibiotics.
Warning
Starting corticosteroids or antibiotics before DAT confirmation is premature and may obscure the diagnosis. DAT must be done first to guide specific therapy (corticosteroids for warm AIHA, cold avoidance for cold AIHA, plasmapheresis for severe cases).
Robbins 10e Ch 13
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.