Anemias Overview MCQ — NEET PG Practice Question | NEETPGAI
Anemias Overview
medium
microscope Pathology
A 52-year-old man with chronic kidney disease (eGFR 28 mL/min/1.73m²) presents with fatigue and dyspnea. His hemoglobin is 7.8 g/dL, MCV 82 fL, reticulocyte count 1.2% (normal 0.5–2.5%). Iron studies are normal. What is the most appropriate next step in management?
A. Perform bone marrow biopsy to assess erythropoiesis
B. Initiate erythropoiesis-stimulating agent (ESA) therapy
C. Measure serum erythropoietin (EPO) level
D. Start iron supplementation to optimize iron stores
Explanation
Clinical Diagnosis
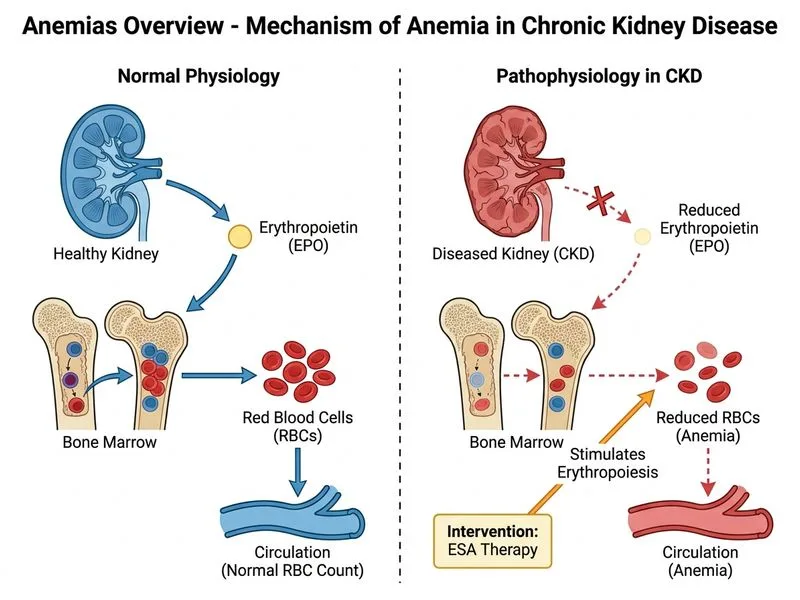
The patient has normocytic anemia (MCV 82 fL) with low reticulocyte count (1.2%) in the setting of chronic kidney disease (CKD). Normal iron studies exclude iron deficiency. This is anemia of chronic kidney disease (CKD-related anemia), primarily due to EPO deficiency.
Pathophysiology of CKD-Related Anemia
Key Point
In CKD, the kidneys produce <10% of normal EPO, leading to inadequate RBC production despite intact bone marrow function. The reticulocyte count is inappropriately low for the degree of anemia, confirming hypoproliferative anemia.
Management Algorithm for CKD Anemia
Loading diagram...
High-YieldNEET PG
ESA (erythropoietin or darbepoetin alfa) is the first-line pharmacologic therapy for CKD anemia once iron stores are adequate. Do NOT measure serum EPO levels — they are elevated in CKD but remain insufficient to drive erythropoiesis. Clinical response (Hb rise) is the measure of ESA efficacy.
Why NOT Measure EPO Level
Table
Test
CKD Anemia
Rationale
Serum EPO
Elevated (100–500 mIU/mL)
Kidneys cannot produce enough; absolute level is irrelevant
Reticulocyte count
Low/inappropriately normal
Confirms hypoproliferative mechanism
Iron studies
Normal (in this case)
ESA requires iron availability
Bone marrow
Normal
Rules out other causes (aplasia, infiltration)
Clinical Pearl
Measuring serum EPO in CKD is a common misconception. EPO levels are already elevated in CKD; the problem is insufficient production relative to anemia severity. Starting ESA directly based on clinical criteria (Hb <10 g/dL in CKD) is the standard approach.
Tip
Before starting ESA, ensure:
1.
Iron stores adequate (ferritin >100 ng/mL, TSAT >20%)
2.
No active infection or inflammation (CRP, WBC)
3.
Reticulocyte count confirms hypoproliferation
4.
Blood pressure controlled (ESA can raise BP)
Warning
ESA target is Hb 10–12 g/dL in CKD; avoid Hb >13 g/dL due to increased thrombotic risk. Monitor for hypertension and thrombosis.
Harrison 21e Ch 105; KDIGO 2021 Anemia in CKD
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.