## Diagnosis: Anemia of Chronic Disease (ACD) ### Clinical Context The patient has a chronic inflammatory disease (rheumatoid arthritis) of 10 years' duration with systemic manifestations (hepatosplenomegaly), and has developed anemia. This is the classic setting for **anemia of chronic disease**. ### Laboratory Pattern — Diagnostic Hallmark | Parameter | Finding | Interpretation | |-----------|---------|----------------| | **Hemoglobin** | 9.8 g/dL | Mild anemia | | **MCV** | 78 fL | Normocytic to slightly microcytic | | **RBC morphology** | Normal | No hypochromia or target cells | | **Serum ferritin** | 280 ng/mL | **Elevated** (normal < 200) — acute phase reactant | | **Serum iron** | 35 μg/dL | Low | | **TIBC** | 240 μg/dL | **Low** (normal 250–425) — key finding | | **Transferrin saturation** | 15% | Low | | **Peripheral smear** | Normocytic, normal morphology | No hypochromia | **Key Point:** The combination of **elevated ferritin + low TIBC + low serum iron + normal RBC morphology** is pathognomonic for anemia of chronic disease. The low TIBC distinguishes ACD from iron deficiency anemia. ### Pathophysiology of ACD In chronic inflammation (RA, infection, malignancy, autoimmune disease), the following occurs: 1. **Hepcidin upregulation**: IL-6 and TNF-α stimulate hepcidin production 2. **Iron sequestration**: Hepcidin blocks ferroportin on macrophages → iron trapped in reticuloendothelial system 3. **Reduced erythropoietin response**: Blunted EPO production relative to degree of anemia 4. **Shortened RBC survival**: Mild hemolysis from chronic inflammation 5. **Result**: Functional iron deficiency with iron-replete stores ### Why TIBC is Low (Critical Discriminator) - **Iron deficiency anemia**: TIBC is **elevated** (> 425 μg/dL) because the body upregulates transferrin production to maximize iron transport - **Anemia of chronic disease**: TIBC is **low** (< 250 μg/dL) because transferrin synthesis is suppressed by inflammation **High-Yield:** TIBC is the single most useful test to differentiate iron deficiency anemia from anemia of chronic disease when both present with low serum iron. ### Why Ferritin is Elevated Ferritin is an acute phase reactant — it rises with inflammation regardless of iron status. In RA, ferritin is often markedly elevated due to ongoing synovial inflammation. **Clinical Pearl:** Hepatosplenomegaly in this patient likely reflects extramedullary hematopoiesis and iron deposition in the reticuloendothelial system, consistent with iron sequestration in ACD. ### Comparison Table: Iron Deficiency vs. ACD | Feature | Iron Deficiency | ACD | |---------|-----------------|-----| | **Ferritin** | ↓↓ (< 30) | ↑ (> 200) | | **Serum iron** | ↓ | ↓ | | **TIBC** | ↑↑ (> 425) | ↓ (< 250) | | **Transferrin sat.** | ↓ | ↓ | | **RBC morphology** | Microcytic, hypochromic | Normocytic, normal | | **MCV** | < 80 | 80–100 | | **Cause** | Blood loss, malabsorption | Chronic inflammation | **Mnemonic: FERRITIN in ACD** — **F**erritin ↑, **E**PO response blunted, **R**eticuloendothelial iron sequestration, **R**BC survival ↓, **I**ron trapped, **T**IBC ↓, **I**nflammation present, **N**ormocytic anemia 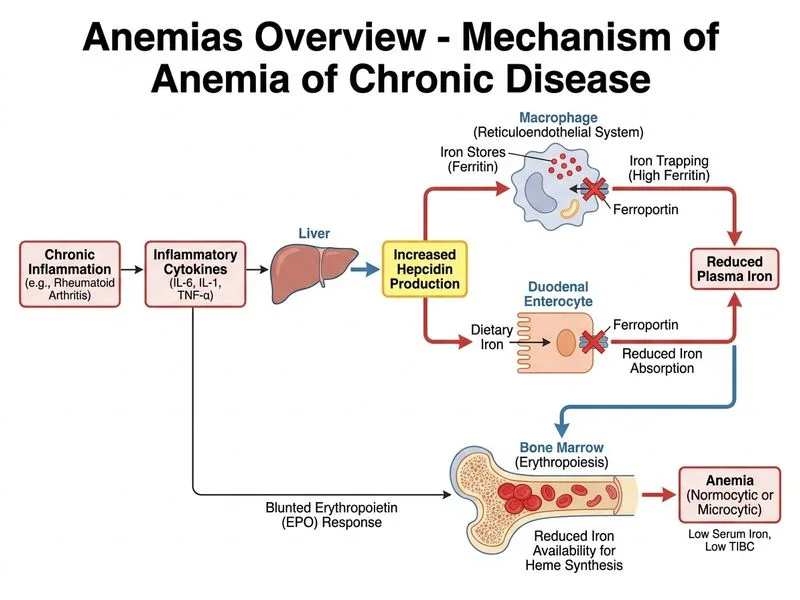
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.