## Morphologic Classification of Anemias **Key Point:** The **Mean Corpuscular Volume (MCV)** is the primary parameter used to classify anemias morphologically into microcytic, normocytic, and macrocytic categories. ### MCV-Based Classification | Classification | MCV Range (fL) | Common Causes | |---|---|---| | **Microcytic** | <80 | Iron deficiency, thalassemia, anemia of chronic disease, sideroblastic anemia | | **Normocytic** | 80–100 | Hemolytic anemia, acute blood loss, bone marrow failure, hemoglobinopathy | | **Macrocytic** | >100 | Megaloblastic (B12/folate deficiency), non-megaloblastic (alcohol, reticulocytosis, liver disease) | **High-Yield:** MCV is the **first-line discriminator** in anemia workup. It narrows the differential diagnosis and guides further investigation (iron studies, B12/folate levels, reticulocyte count, etc.). ### Why MCV? MCV reflects the **average size of circulating RBCs**: - **Low MCV** → small RBCs → impaired hemoglobin synthesis (iron, globin) or abnormal RBC maturation - **Normal MCV** → normal-sized RBCs → RBC destruction, acute loss, or marrow failure - **High MCV** → large RBCs → impaired DNA synthesis (B12/folate) or immature RBC release **Clinical Pearl:** MCV is calculated as: $MCV = \frac{Hematocrit \times 10}{RBC\ count\ (millions/\mu L)}$ **Mnemonic: MCV First** — When evaluating anemia, always start with MCV; it is the morphologic cornerstone of anemia classification. ### Role of MCHC and RDW - **MCHC** (Mean Corpuscular Hemoglobin Concentration): Reflects hemoglobin saturation of RBCs; rarely abnormal in isolation; less useful for classification - **RDW** (Red Cell Distribution Width): Measures variation in RBC size (anisocytosis); helpful for prognosis and detecting mixed anemias but NOT the primary classifier 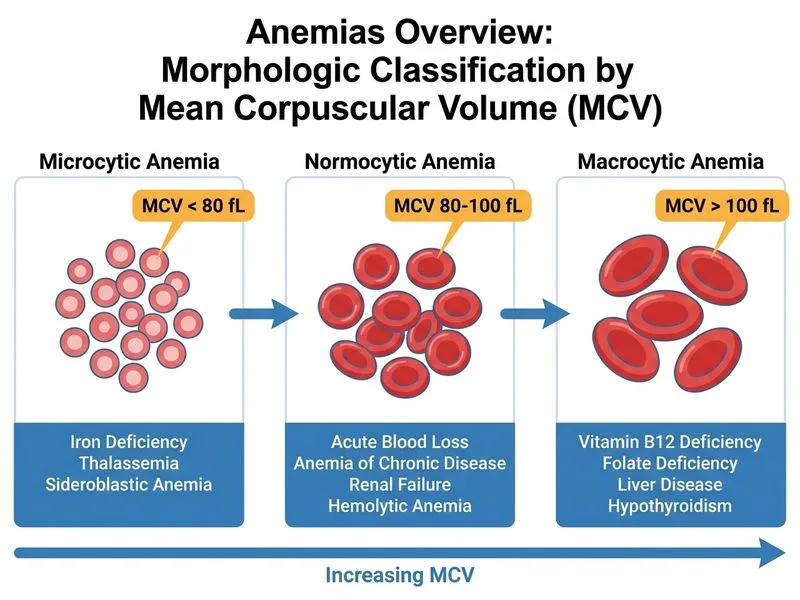
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.