## Diagnosis: Iron Deficiency Anemia ### Clinical Presentation This patient has a classic presentation of iron deficiency anemia (IDA) with: - **Chronic blood loss** from menorrhagia (2 years of heavy periods) - **Progressive symptoms**: fatigue, dyspnea, palpitations - **Physical signs**: pallor, tachycardia, no organomegaly ### Laboratory Findings — The Diagnostic Triad | Parameter | Finding | Interpretation | |-----------|---------|----------------| | **Hemoglobin** | 7.2 g/dL | Moderate anemia | | **MCV** | 62 fL | Microcytic (< 80 fL) | | **MCH** | 18 pg | Hypochromic (< 27 pg) | | **Serum Iron** | 28 µg/dL | **Low** (normal 60–170) | | **Ferritin** | 8 ng/mL | **Very low** (normal 15–200) | | **TIBC** | 420 µg/dL | **Elevated** (normal 250–425) | | **Reticulocyte count** | 1.2% | Inappropriately low for degree of anemia | | **Peripheral smear** | Microcytic hypochromic RBCs, target cells | Consistent with iron lack | **Key Point:** The combination of **low serum iron + low ferritin + elevated TIBC** is pathognomonic for iron deficiency. Ferritin < 15 ng/mL is virtually diagnostic of absent iron stores. ### Pathophysiology 1. Chronic menorrhagia → iron loss exceeds dietary intake 2. Depletion of iron stores → serum ferritin falls 3. Iron-responsive element (IRE) signaling → hepcidin suppression → increased intestinal iron absorption (reflected by high TIBC) 4. Insufficient iron for hemoglobin synthesis → microcytic hypochromic RBCs 5. Blunted reticulocyte response due to iron-limited erythropoiesis ### Morphology of RBCs - **Microcytosis**: MCV < 80 fL (here 62 fL) - **Hypochromia**: MCH < 27 pg (here 18 pg) - **Target cells** (codocytes): central staining due to reduced hemoglobin content - **Pencil cells** (anisopoikilocytosis): variation in RBC size and shape **High-Yield:** In IDA, the **reticulocyte count is inappropriately low** relative to the degree of anemia — bone marrow cannot compensate because it lacks iron substrate for hemoglobin synthesis. This distinguishes IDA from hemolytic anemias (where reticulocyte count is elevated). **Clinical Pearl:** The source of bleeding must be identified. In a premenopausal woman with menorrhagia, gynecologic evaluation is essential; however, GI bleeding (occult or overt) must also be ruled out in any IDA patient, especially if iron supplementation fails to correct the anemia. ### Management Approach 1. **Confirm diagnosis**: serum iron, ferritin, TIBC, peripheral smear 2. **Identify source**: menstrual history, GI evaluation (fecal occult blood, upper/lower endoscopy if indicated) 3. **Iron replacement**: oral ferrous sulfate 325 mg daily (or IV iron if malabsorption/intolerance) 4. **Monitor**: repeat CBC in 4–6 weeks; expect Hb rise of 1–2 g/dL per month 5. **Address underlying cause**: treat menorrhagia (hormonal therapy, IUD, surgical intervention) or GI pathology 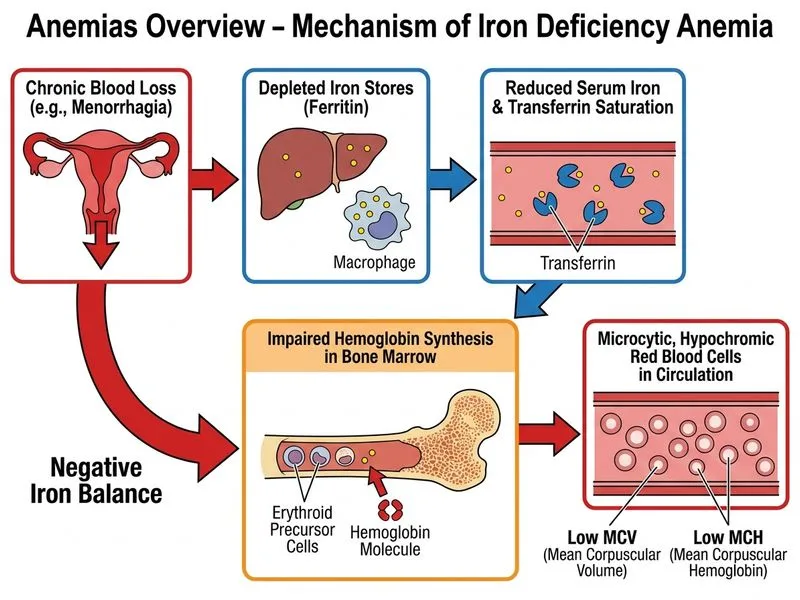
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.