## Diagnosis: Anemia of Chronic Disease (from Rheumatoid Arthritis) ### Clinical Context This patient has: - **Rheumatoid arthritis (RA)** for 15 years — a well-established cause of anemia of chronic disease (ACD) - **Anemia**: Hb 8.5 g/dL, normocytic to mildly microcytic (MCV 78 fL) - **Iron studies consistent with ACD**: normal-high ferritin, normal serum iron, low-normal TIBC - **CKD Stage 3b** (eGFR 42 mL/min): present but NOT the primary driver of anemia here ### Why Anemia of Chronic Disease (ACD) is the Best Answer #### Iron Studies Are the Key Discriminator | Parameter | This Patient | IDA Pattern | ACD Pattern | CKD Anemia | |-----------|--------------|-------------|-------------|------------| | **Serum Iron** | 85 µg/dL | Low (< 60) | Low-normal ✓ | Normal | | **Ferritin** | 180 ng/mL | Low (< 15) | **Normal-high ✓** | Normal | | **TIBC** | 280 µg/dL | Elevated (> 425) | **Low-normal ✓** | Normal | | **Reticulocyte** | 0.8% | Low | Low ✓ | Low | **Key Point:** The combination of **normal-high ferritin (180 ng/mL)** + **low-normal TIBC (280 µg/dL)** + **normal serum iron** is the classic hallmark of **ACD**, not CKD anemia. In ACD, hepcidin sequesters iron in macrophages (ferritin rises, TIBC falls), whereas in pure CKD anemia, iron studies are typically normal. ### Pathophysiology of ACD in RA 1. **Chronic inflammation** → IL-6, TNF-α, IL-1 elevation (all elevated in RA) 2. **IL-6 → hepatic hepcidin synthesis** → hepcidin blocks ferroportin → iron trapped in macrophages/hepatocytes 3. **Result**: Serum iron falls (functional iron deficiency), ferritin rises (iron stored), TIBC falls (transferrin synthesis suppressed) 4. **Cytokine-mediated EPO suppression**: TNF-α and IL-1 blunt EPO production and erythroid progenitor response 5. **Shortened RBC lifespan**: Inflammatory cytokines reduce RBC survival 6. **Net effect**: Normocytic (sometimes mildly microcytic) anemia with low reticulocyte count *(Robbins & Cotran Pathologic Basis of Disease, 10th ed., Chapter on Red Cell Disorders; Harrison's Principles of Internal Medicine, 21st ed., Chapter 99)* ### Why CKD Anemia (Option D) is Less Likely Here - **CKD anemia** (EPO deficiency) is typically **normocytic** (MCV 80–90 fL) with **normal iron studies** — ferritin, serum iron, and TIBC are all within normal range - The **low-normal TIBC (280 µg/dL)** and **ferritin 180 ng/mL** are NOT characteristic of pure CKD anemia; they point to inflammatory iron sequestration - eGFR 42 mL/min (Stage 3b) can contribute to anemia, but EPO deficiency typically becomes clinically significant at eGFR < 30 mL/min (Stage 4–5) - The **15-year history of RA** is a far more established and dominant cause of ACD than Stage 3b CKD - **Clinical Pearl (Harrison's):** When CKD and chronic inflammation coexist, the iron study pattern (low TIBC, high ferritin) favors ACD as the primary mechanism ### Why Other Options Are Incorrect **Option A — Sideroblastic Anemia from Methotrexate:** - Methotrexate causes **megaloblastic (macrocytic) anemia** via folate antagonism, NOT sideroblastic anemia - Sideroblastic anemia shows **markedly elevated serum iron and ferritin** (iron overload pattern) with ringed sideroblasts on bone marrow biopsy — none of these features are present - MCV here is 78 fL (microcytic/normocytic), not macrocytic **Option C — Iron Deficiency Anemia from NSAID-induced GI Bleeding:** - IDA requires **low ferritin (< 15 ng/mL)** and **elevated TIBC (> 425 µg/dL)** - This patient has ferritin 180 ng/mL and TIBC 280 µg/dL — both inconsistent with IDA - A single ferritin > 100 ng/mL effectively excludes iron deficiency as the primary cause **Option D — Anemia of CKD:** - As discussed, Stage 3b CKD contributes but does NOT explain the low TIBC and high-normal ferritin - ACD from RA is the dominant mechanism supported by the iron study pattern ### Management Implications 1. **Treat underlying RA**: DMARDs (methotrexate already on board), biologics (anti-TNF) reduce inflammation → improve ACD 2. **Iron supplementation**: NOT indicated (ferritin adequate, TIBC not elevated) 3. **ESA**: Consider only if EPO levels are disproportionately low; not first-line for ACD 4. **Monitor renal function**: CKD management (ACE inhibitor, glycemic control) to prevent progression **High-Yield:** In ACD, the **ferritin is normal-to-high** and **TIBC is low-to-normal** — the opposite of IDA. This pattern reflects hepcidin-mediated iron sequestration driven by chronic inflammation (RA, malignancy, chronic infection). *(KD Tripathi Essentials of Medical Pharmacology; Robbins Pathology)* 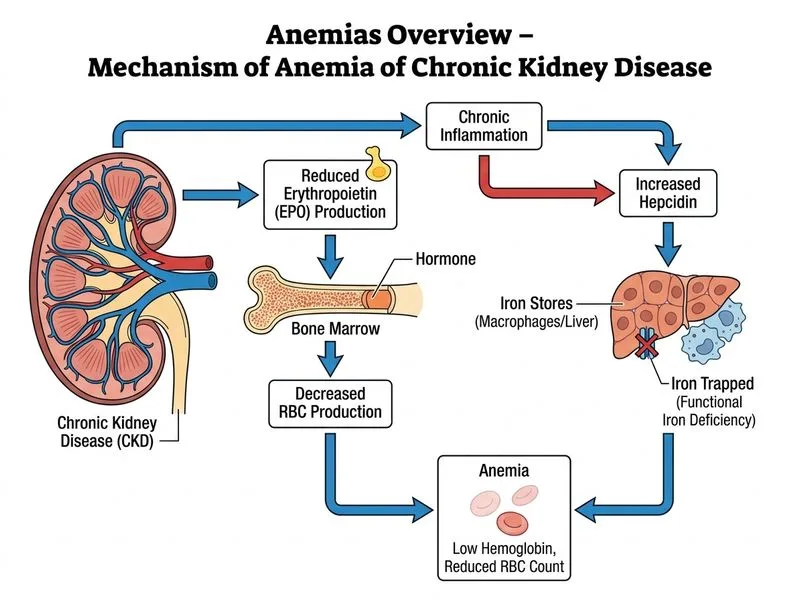
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.