## Clinical Diagnosis: Acute Severe Asthma Exacerbation (Status Asthmaticus) ### Key Point: **This patient has life-threatening asthma exacerbation with impending respiratory failure (hypercapnia, acidosis, poor air entry, inability to speak).** ## Severity Assessment | Feature | Finding | Severity Grade | |---------|---------|----------------| | Dyspnea | Cannot complete sentences | **Severe** | | Respiratory rate | 32/min | Tachypneic | | SpO₂ | 88% on room air | **Hypoxemia** | | PEF | 180 L/min (33% predicted) | **<40% = severe** | | Air entry | Poor bilaterally, silent zones | **Impending respiratory failure** | | pH | 7.28 | **Respiratory acidosis** | | PaCO₂ | 52 mmHg | **Hypercapnia (>45 = danger sign)** | | Response to SABA | No relief after 6 hours | **Refractory exacerbation** | **High-Yield:** - **Hypercapnia (PaCO₂ >45) in acute asthma = DANGER SIGN of impending respiratory failure** - **Respiratory acidosis (pH <7.35 + PaCO₂ >45) = requires ICU-level care** - Silent chest + inability to speak + hypercapnia = consider intubation if no rapid response ## Acute Severe Asthma Management Algorithm ```mermaid flowchart TD A[Acute severe asthma exacerbation]:::outcome --> B[Assess severity: ABG, PEF, SpO2, air entry]:::action B --> C{Hypercapnia or respiratory acidosis?}:::decision C -->|No: PaCO2 <45, pH >7.35| D[Step 1: Oxygen + SABA + ICS + Mg2+]:::action C -->|Yes: PaCO2 >45, pH <7.35| E[Step 1: Oxygen + SABA + ICS + IV Mg2+]:::action E --> F[Add ipratropium to SABA nebulization]:::action F --> G[Prepare for ICU admission]:::action D --> H{Response in 1-2 hours?}:::decision E --> H H -->|Good: PEF >50%, SpO2 >90%| I[Continue therapy, admit to ward]:::outcome H -->|Poor: PEF <50%, SpO₂ <90%| J[ICU admission, consider intubation]:::urgent ``` ## Immediate Management (First 1–2 Hours) ### 1. **Oxygen Therapy** - Target SpO₂ ≥90–92% (avoid excessive oxygen which may suppress respiratory drive in CO₂ retainers) - This patient needs high-flow oxygen given SpO₂ 88% ### 2. **Bronchodilators** - **Nebulized salbutamol:** 5 mg (or 10 mg in severe cases) every 15–20 minutes for first hour, then every 1–4 hours - **Nebulized ipratropium:** 0.5 mg added to salbutamol (anticholinergic; synergistic with beta-agonist) - Combination SABA + anticholinergic is superior to SABA alone in severe exacerbations ### 3. **Systemic Corticosteroids** (IV preferred in severe exacerbation) - **IV methylprednisolone:** 125 mg (or equivalent IV hydrocortisone 500 mg) immediately, then 6-hourly - Oral prednisolone 40–50 mg is acceptable if IV access difficult, but IV is preferred in severe cases - **Do NOT delay steroids waiting for response to bronchodilators** ### 4. **IV Magnesium Sulfate** - **Dose:** 2 g IV over 20 minutes (or 1–2 g over 5–10 minutes if very severe) - Mechanism: Smooth muscle relaxant; particularly effective in refractory exacerbations - **Indication:** Severe exacerbations with poor response to initial SABA therapy ### 5. **Reassessment at 1–2 Hours** - Repeat PEF, SpO₂, ABG - If **no improvement or worsening:** ICU admission, continuous nebulization, consider IV aminophylline, and prepare for intubation - If **improvement:** Continue therapy, admit to high-dependency unit or ward **Clinical Pearl:** The presence of **hypercapnia with respiratory acidosis** in acute asthma is a sign of **severe airflow obstruction with respiratory muscle fatigue**. This patient is at imminent risk of respiratory arrest and requires: 1. Aggressive bronchodilation (SABA + anticholinergic) 2. High-dose IV corticosteroids 3. IV magnesium sulfate 4. **Continuous monitoring with low threshold for ICU admission and intubation** ## Why Not Intubation Immediately (Option 4)? - **Medical therapy should be given a trial first** (1–2 hours) unless the patient is in immediate respiratory arrest - Intubation in asthma is **high-risk** (difficult to ventilate, risk of auto-PEEP and barotrauma, prolonged weaning) - Many patients respond to aggressive medical therapy and can avoid intubation - **Indications for intubation:** Respiratory arrest, severe hypoxemia unresponsive to oxygen, exhaustion, inability to protect airway ## Why Not Option 1 (Magnesium Omitted)? - This patient has a **refractory exacerbation** (no response to SABA for 6 hours) and **hypercapnia with acidosis** - IV magnesium sulfate is indicated in severe exacerbations and significantly improves outcomes - Omitting magnesium in this high-risk scenario is suboptimal ## Why Not Option 3 (Oral Prednisolone Only)? - **Oral corticosteroids are inadequate for severe exacerbations** with hypercapnia and respiratory acidosis - **IV corticosteroids are preferred** because they achieve higher serum levels faster - This patient requires ICU-level monitoring, not discharge home - Oral therapy is only appropriate for mild-to-moderate exacerbations managed in primary care or ED observation **Mnemonic:** **SABA-IC** for Severe Asthma Exacerbation - **S**albutamol (nebulized, frequent) - **A**nticholinergic (ipratropium) - **B**ronchodilator support (continuous) - **A**irway assessment (prepare for intubation) - **I**V corticosteroids (methylprednisolone) - **C**ontinuous magnesium sulfate [cite:Harrison 21e Ch 242; GINA 2023 Global Strategy for Asthma Management and Prevention] 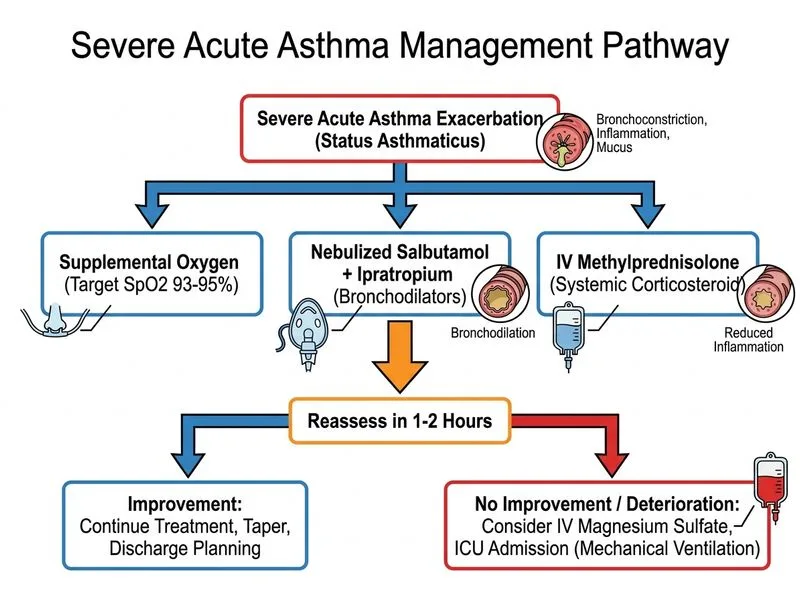
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.