## Breakthrough Pain Management in Opioid-Tolerant Patients **Correct Answer: Switch to transdermal fentanyl 75 mcg/72 h and add immediate-release opioid for breakthrough pain** ### Rationale: This patient has **opioid-tolerant cancer pain** with inadequate control on 180 mg/day oral morphine. The standard approach for breakthrough pain in this setting involves: 1. **Conversion to long-acting formulation (transdermal fentanyl):** - Fentanyl 75 mcg/72 h is approximately equianalgesic to morphine 180 mg/day (using the 1:100 conversion ratio for opioid-naïve patients; for tolerant patients, conversion is individualized but fentanyl offers superior pharmacokinetics) - Transdermal delivery provides stable, continuous analgesia - Reduces fluctuations in serum levels that drive breakthrough pain 2. **Addition of immediate-release opioid for breakthrough pain:** - Typically 10–20% of total daily opioid dose given as IR formulation (e.g., morphine IR 15–30 mg, or fentanyl lozenge 200–400 mcg) - Addresses acute exacerbations without increasing baseline dosing - This is the **gold standard** per WHO analgesic ladder and cancer pain guidelines (ASCO, NCCN) 3. **Consideration of adjuvants:** - Neuropathic components (bone pain often has neuropathic features) may benefit from gabapentin, pregabalin, or duloxetine *in addition to* opioid optimization, not as replacement **Key Point:** The goal is NOT to increase baseline morphine dose further (risk of toxicity) but to optimize delivery kinetics and add targeted breakthrough coverage. --- ## Why Each Distractor Is Wrong: **Option 0: Increase oral morphine by 50% + NSAID** - Escalating oral morphine when already on 180 mg/day increases risk of constipation, cognitive impairment, and respiratory depression - NSAIDs are contraindicated or high-risk in advanced cancer (GI bleeding, renal compromise, platelet dysfunction) - Does NOT address the pharmacokinetic problem of breakthrough pain (fluctuating serum levels) **Option 2: Add gabapentin + reduce morphine by 25%** - Gabapentin is an adjuvant for neuropathic pain, NOT a substitute for opioid escalation in inadequately controlled cancer pain - Reducing morphine while pain is uncontrolled is counterintuitive and harmful - Gabapentin should be *added* to optimized opioid therapy, not used to replace it **Option 3: Initiate methadone monotherapy with abrupt morphine discontinuation** - Methadone is a valid alternative opioid but requires **slow, careful titration** (risk of QT prolongation, drug interactions, accumulation) - **Abrupt discontinuation of morphine** risks acute withdrawal and loss of analgesia - Methadone conversion is typically reserved for opioid-induced side effects or tolerance, not first-line for breakthrough pain - Requires ICU/high-dependency monitoring in many settings --- ## High-Yield Concepts: | Aspect | Detail | |--------|--------| | **Breakthrough pain definition** | Transient exacerbation of pain in opioid-tolerant patients on stable baseline therapy | | **First-line management** | Optimize long-acting formulation + add IR opioid (10–20% total daily dose) | | **Transdermal fentanyl advantage** | Steady-state levels, reduced fluctuation, lower GI side effects than oral morphine | | **Adjuvants** | Add (don't replace) for neuropathic/bone pain: gabapentin, pregabalin, duloxetine, NSAIDs (if safe) | | **Methadone role** | Rescue option for intolerable side effects or drug interactions; NOT first-line | **Clinical Pearl:** In cancer pain, the "ceiling" for opioid escalation is determined by toxicity, not efficacy. Once toxicity limits further dose increase, switch strategy (formulation, add adjuvants, consider interventional approaches like nerve blocks). 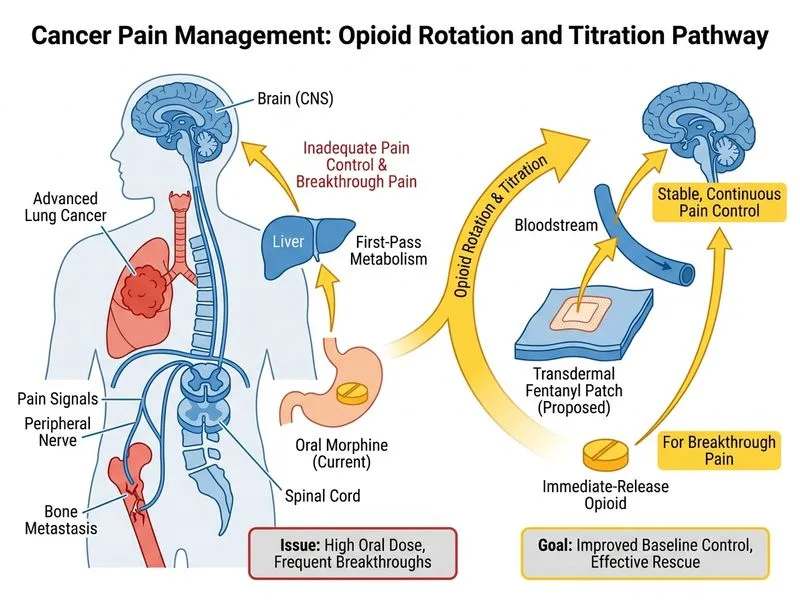
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.