A 52-year-old man with chronic hypertension presents with left ventricular hypertrophy on echocardiography. His colleague, a 48-year-old bodybuilder, has physiologic hypertrophy of skeletal muscle from resistance training. Which feature best distinguishes pathologic cardiac hypertrophy from physiologic skeletal muscle hypertrophy?
A. Preserved or enhanced contractile function and oxygen delivery capacity
B. Increase in individual cell size without increase in cell number
C. Activation of fetal gene program and increased collagen deposition
D. Reversibility upon removal of the stimulus
Explanation
Distinguishing Pathologic vs. Physiologic Hypertrophy
Key Structural Difference
Key Point
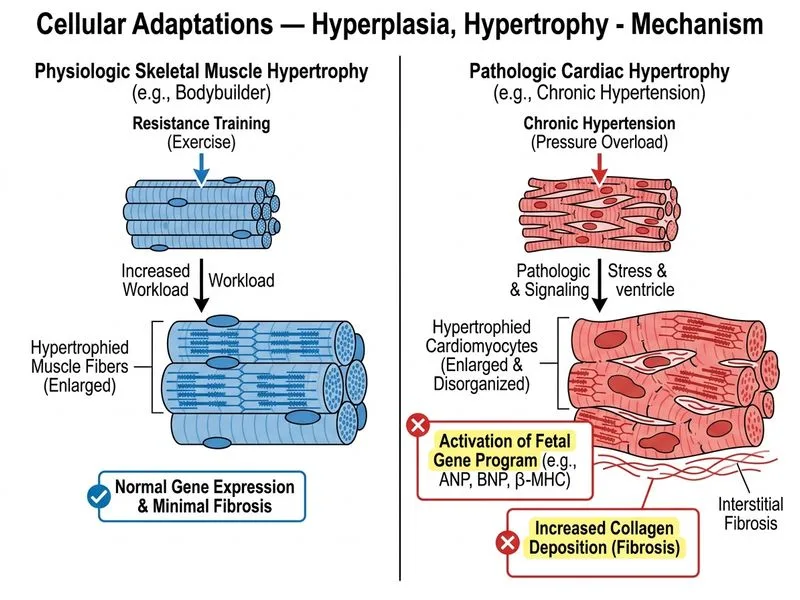
Pathologic hypertrophy is characterized by activation of the fetal gene program (increased expression of β-myosin heavy chain, atrial natriuretic peptide, and α-skeletal actin) and progressive interstitial fibrosis, whereas physiologic hypertrophy maintains normal gene expression patterns.
The fetal gene program activation (β-MHC, ANP, α-skeletal actin) is the hallmark that distinguishes pathologic from physiologic hypertrophy and predicts progression to heart failure.
Clinical Pearl
Pathologic LV hypertrophy in hypertension initially compensates for increased afterload but eventually leads to diastolic dysfunction, then systolic dysfunction and heart failure — a progression that does not occur in physiologic muscle hypertrophy.
Why Collagen Deposition Matters
Progressive fibrosis in pathologic hypertrophy:
Increases myocardial stiffness
Impairs electrical conduction
Reduces coronary perfusion relative to mass
Becomes irreversible even if the original stimulus (e.g., hypertension) is controlled
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.