## Clinical Context This patient has a history of genital HSV but no active lesions or prodromal symptoms at the time of labour. The key distinction in HSV management during pregnancy is whether there are active lesions or prodromal symptoms at delivery. ## Indications for Cesarean Section in HSV | Finding | Management | |---------|-------------| | **Active herpetic lesions at delivery** | Cesarean section (to prevent neonatal transmission) | | **Prodromal symptoms (pain, tingling, burning)** | Cesarean section | | **History of HSV but no active lesions/prodrome** | Vaginal delivery is safe; prophylactic IV acyclovir recommended | | **First episode of HSV in third trimester** | Cesarean section | **Key Point:** The risk of neonatal herpes transmission is highest (30–50%) with primary HSV infection at delivery, moderate (3–5%) with recurrent infection with active lesions, and <1% with recurrent infection without lesions. **High-Yield:** Absence of active lesions or prodromal symptoms in a patient with recurrent HSV history makes vaginal delivery safe. Prophylactic IV acyclovir (5 mg/kg IV every 8 hours) is given during labour to further reduce transmission risk. **Clinical Pearl:** Many clinicians unnecessarily perform cesarean sections for HSV history alone. The 2020 ACOG guidelines and RCOG recommendations emphasize that vaginal delivery is appropriate if there are no active lesions or prodromal symptoms, regardless of serology or past history. ## Why Vaginal Delivery is Safe Here 1. No active lesions on examination 2. No prodromal symptoms reported 3. Last clinical episode was 8 months ago (recurrent, not primary) 4. Prophylactic acyclovir further reduces risk [cite:ACOG Practice Bulletin 82] 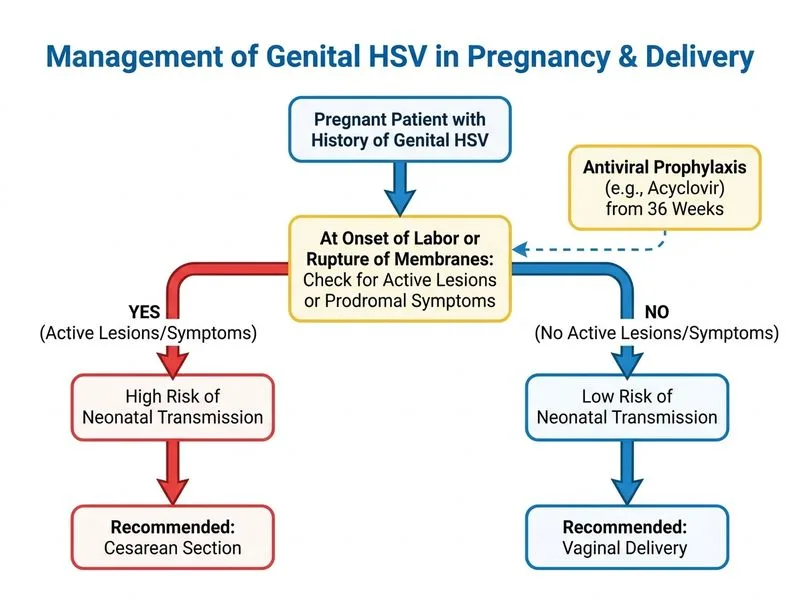
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.