## Clinical Scenario Analysis This patient has **complete placenta previa** (placental edge ≤2 cm from internal os) with: - Stable hemodynamics - Mild anemia (Hb 10.2 g/dL) — acceptable for expectant management - No active labor - Reassuring fetal status - Proximity to hospital (2 km) ## Management of Placenta Previa by Presentation | Feature | Expectant Management | Immediate Cesarean | |---------|----------------------|--------------------| | **Hemodynamic stability** | Required | Not required | | **Fetal maturity** | Preferred (≥34 wks) | Not required | | **Active bleeding** | Minimal/resolved | Ongoing/massive | | **Maternal proximity to hospital** | Essential | Not critical | | **Maternal preference** | Considered | Overridden if unstable | ## High-Yield Management Algorithm ```mermaid flowchart TD A[Placenta Previa diagnosed]:::outcome --> B{Maternal hemodynamics stable?}:::decision B -->|No - Unstable| C[Immediate cesarean]:::urgent B -->|Yes - Stable| D{Gestational age ≥ 34 weeks?}:::decision D -->|No| E[Admit for observation + corticosteroids]:::action D -->|Yes| F[Admit for expectant management]:::action F --> G{Bleeding episode during admission?}:::decision G -->|Yes - massive| H[Cesarean immediately]:::urgent G -->|No or minor| I[Plan elective cesarean at 39 weeks]:::action E --> J[Reassess at 34 weeks]:::action ``` ## Key Point: **Expectant management is the standard of care** for hemodynamically stable patients with placenta previa at ≥34 weeks gestation. Elective cesarean is planned at 39 weeks or earlier if bleeding recurs. ## Clinical Pearl: - **Admission is mandatory** even if stable, because placenta previa can bleed unpredictably - **Pelvic rest** (no intercourse, no digital cervical exams) is enforced - **Corticosteroids** are NOT indicated at 38 weeks (fetal lungs mature) - **Vaginal delivery is contraindicated** in complete previa; cesarean is inevitable ## Why Expectant Management Here? 1. Patient is hemodynamically stable 2. Gestational age 38 weeks (fetal lungs mature) 3. Lives near hospital (can reach quickly if bleeding resumes) 4. No active hemorrhage at presentation 5. Allows completion of 39 weeks for optimal neonatal outcomes ## Why NOT immediate cesarean? Immediate cesarean is reserved for **hemodynamic instability, massive bleeding, or fetal distress**. This patient is stable and can safely await elective cesarean at 39 weeks with close inpatient monitoring. [cite:ACOG Practice Bulletin 208; Cunningham 26e Ch 34] 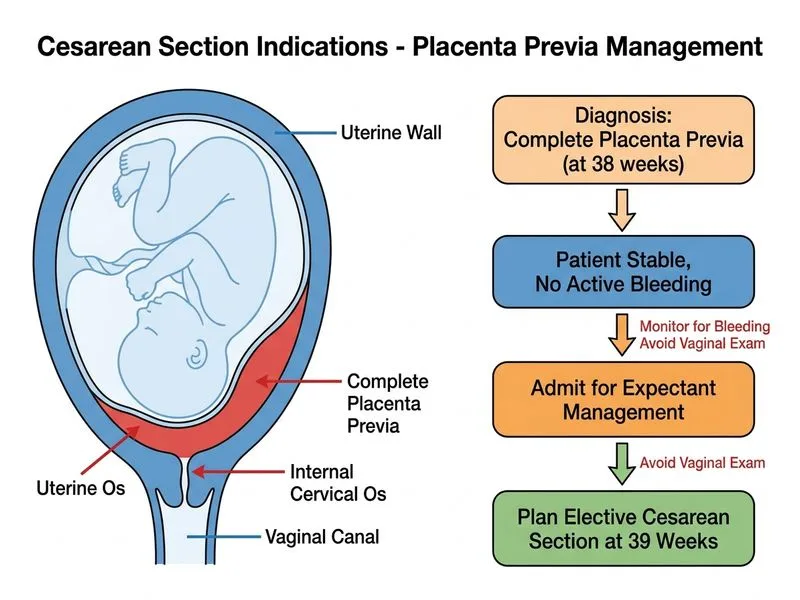
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.