## Clinical Context This patient has stage 4 CKD (eGFR 15–29 mL/min/1.73m²) secondary to diabetic nephropathy, evidenced by long-standing diabetes, proteinuria, normal-sized kidneys with increased echogenicity, and progressive renal dysfunction. ## Management Rationale **Key Point:** Stage 4 CKD management focuses on slowing progression, managing complications, and preparing for renal replacement therapy—NOT immediate dialysis. ### Pharmacological Interventions | Intervention | Indication | Rationale | |---|---|---| | ACE inhibitor or ARB | Hypertension + proteinuria | Reduces intraglomerular pressure, slows GFR decline | | Phosphate binder (calcium-based or non-calcium) | Serum phosphate 4.8 mg/dL | Prevents secondary hyperparathyroidism and vascular calcification | | Erythropoiesis-stimulating agent (ESA) | Hemoglobin 9.2 g/dL (anemia of CKD) | Target Hb 10–11.5 g/dL; avoid overshooting to prevent thrombosis | | Calcium supplementation | Serum calcium 8.2 mg/dL | Correct hypocalcemia; monitor with phosphate | **High-Yield:** At eGFR 18, the patient is NOT yet on dialysis (dialysis typically initiated at eGFR < 10–15 or when symptomatic uremia develops). However, vascular access should be created and patient counseled on dialysis modalities. ### Non-Pharmacological Measures - **Renal diet:** Protein restriction (0.6–0.8 g/kg/day), sodium < 2 g/day, potassium restriction (given K⁺ 5.8) - **Fluid restriction:** As kidney function declines - **Blood pressure control:** Target < 130/80 mmHg (KDIGO 2021) - **Glycemic control:** HbA1c target 7–8% to avoid hypoglycemia in advanced CKD **Clinical Pearl:** Preparation for renal replacement therapy (education on hemodialysis, peritoneal dialysis, transplantation) should begin at stage 4 CKD, but dialysis initiation is determined by symptomatology, residual renal function, and metabolic markers—not eGFR alone. ## Why This Approach? The combination of ACE inhibitor (renoprotection + BP control), phosphate binder (prevent mineral bone disease), and ESA (correct anemia) addresses the three major complications of advanced CKD: progressive renal dysfunction, secondary hyperparathyroidism, and anemia. Dietary counseling and fluid restriction optimize metabolic control and delay need for dialysis. [cite:Harrison 21e Ch 279] 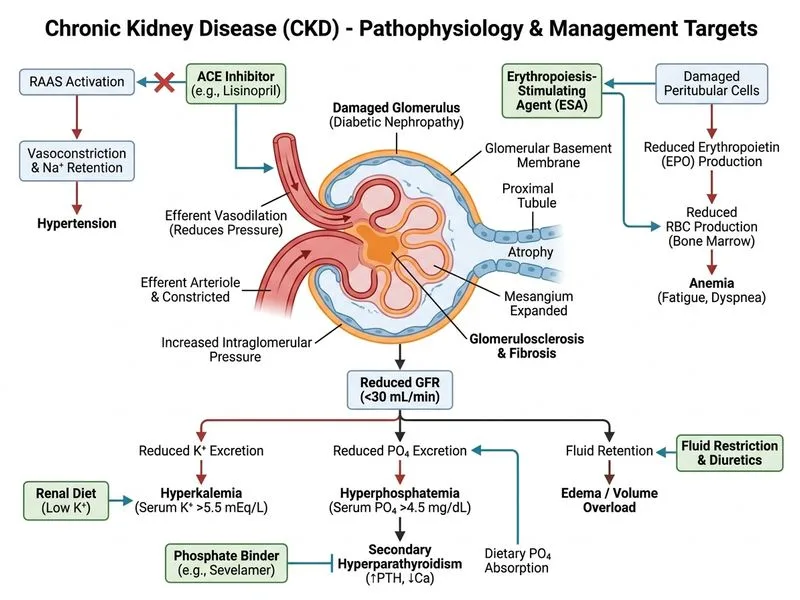
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.