## Clinical Presentation Analysis This patient presents with a constellation of findings consistent with **acute decompensated heart failure (ADHF) superimposed on chronic kidney disease**, resulting in acute-on-chronic kidney injury (AKI): ### Key Clinical Features **Cardiac Findings:** - Dyspnea, orthopnea, peripheral edema (classic heart failure triad) - Elevated JVP and bibasilar crackles (pulmonary edema) - Elevated BNP (650 pg/mL, normal <100 pg/mL) — highly sensitive for heart failure - Chest X-ray confirms pulmonary edema **Renal Findings:** - Acute rise in creatinine (1.8 → 2.4 mg/dL in 2 weeks) on background of CKD Stage 3b - Mild hyponatremia (132 mEq/L) — seen in ADHF due to SIADH and volume overload - Mild hyperkalemia (5.2 mEq/L) — reduced GFR + aldosterone activation - Metabolic acidosis (HCO₃⁻ 18 mEq/L) — tissue hypoperfusion - Preserved urine output with mild proteinuria (2+) — NOT nephritic pattern (no hematuria) **Imaging:** - Normal-sized kidneys with preserved echogenicity — excludes chronic intrinsic renal disease as primary pathology - No hydronephrosis — rules out obstructive uropathy ## Pathophysiology **High-Yield:** In ADHF, reduced cardiac output triggers: 1. Activation of renin-angiotensin-aldosterone system (RAAS) → sodium retention and volume expansion 2. Sympathetic nervous system activation → renal vasoconstriction 3. Reduced renal perfusion pressure → decreased GFR ("cardiorenal syndrome") 4. Fluid accumulation in lungs and periphery **Key Point:** The acute worsening of renal function in the setting of volume overload (not volume depletion) is the hallmark of cardiorenal syndrome, which is distinct from prerenal or intrinsic renal disease. ## Diagnostic Approach ```mermaid flowchart TD A[Dyspnea + Edema + Rising Cr]:::outcome --> B{Elevated BNP?}:::decision B -->|Yes| C[Heart Failure likely]:::action B -->|No| D[Consider other causes] C --> E{Urine findings?}:::decision E -->|Proteinuria only, no RBCs| F[Cardiorenal syndrome]:::outcome E -->|RBCs + Casts| G[Glomerulonephritis]:::outcome E -->|Eosinophiluria + Rash| H[Interstitial nephritis]:::outcome F --> I[Diuretics + ACE-I/ARB + Cardiology consult]:::action ``` ## Why Not the Other Options? | Option | Why Incorrect | |--------|---------------| | **Acute glomerulonephritis** | Acute GN typically presents with active urinary sediment (RBCs, RBC casts, dysmorphic RBCs), hypertension, and rapid rise in creatinine. This patient has proteinuria WITHOUT hematuria or casts — not consistent with GN. Also, BNP would not be elevated. | | **Acute tubular necrosis (ATN)** | ATN from contrast-induced nephropathy typically occurs within 24–72 hours of contrast exposure (no history given). Urine would show muddy-brown casts and high fractional excretion of sodium (FENa >2%). The clinical picture of pulmonary edema and elevated BNP is not typical of ATN. | | **Acute interstitial nephritis (AIN)** | AIN presents with fever, rash, and eosinophiluria ("classic triad"). Urinalysis would show eosinophils and white cell casts, NOT just proteinuria. No history of drug exposure or systemic disease is mentioned. BNP would be normal. | **Clinical Pearl:** Cardiorenal syndrome (Type 1: acute decompensated heart failure with worsening renal function) is a common cause of AKI in hospitalized patients. Management focuses on diuretics to reduce congestion while maintaining renal perfusion, combined with ACE-I/ARB and beta-blockers for cardioprotection. [cite:Harrison 21e Ch 273; Braunwald's Heart Disease 12e Ch 24] 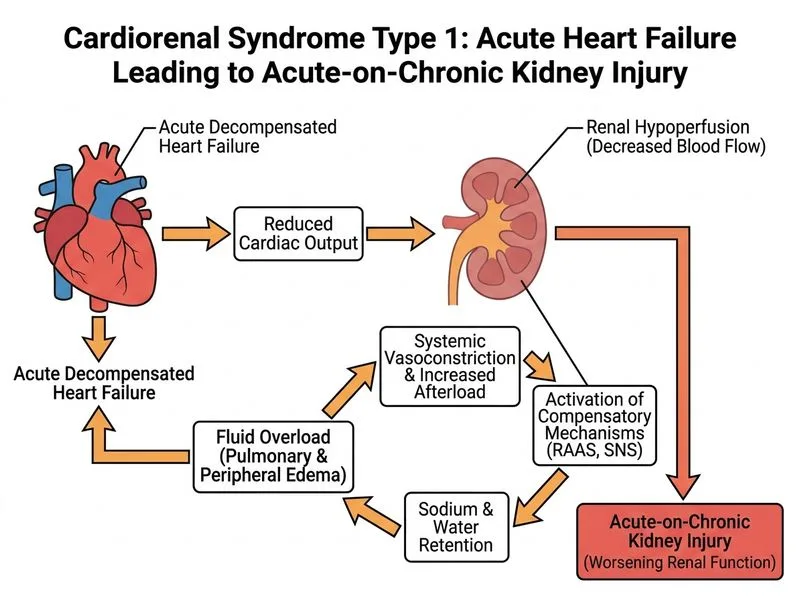
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.