Chronic Leukemias MCQ — NEET PG Practice Question | NEETPGAI
Chronic Leukemias
medium
microscope Pathology
A 62-year-old woman from Mumbai with a 3-year history of chronic lymphocytic leukemia (CLL) presents with progressive lymphadenopathy and splenomegaly. Recent CBC shows lymphocyte count 45,000/µL. Flow cytometry confirms CD5+, CD19+, CD23+ B-cell phenotype. She is asymptomatic with Rai stage II disease and normal renal and hepatic function. Genetic testing shows deletion 13q as the sole abnormality. What is the most appropriate next step in management?
A. Perform TP53 mutation testing and start ibrutinib based on results
B. Start venetoclax monotherapy without further delay
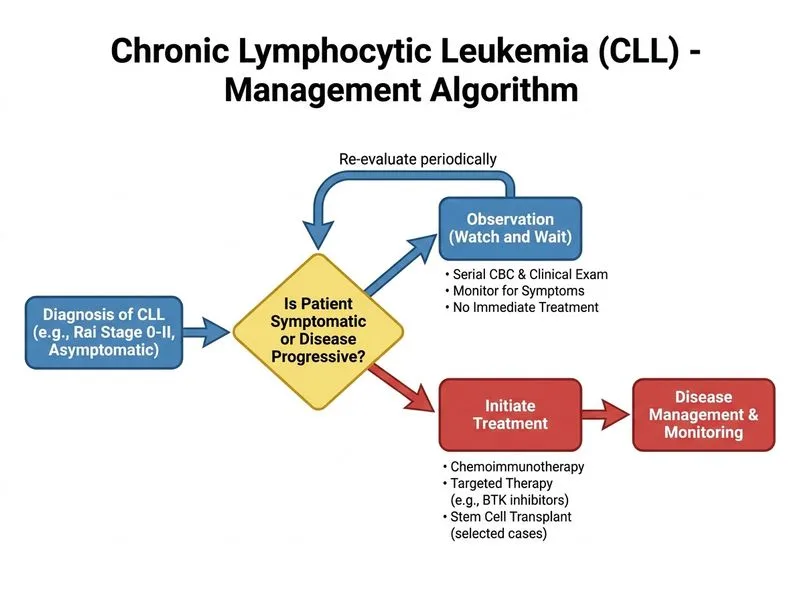
C. Observe with serial CBC and clinical examination; initiate treatment only if symptomatic or progressive disease develops
D. Initiate chemotherapy with fludarabine and cyclophosphamide immediately
Explanation
Watch-and-Wait Strategy in Early-Stage CLL
Key Point
Asymptomatic early-stage CLL (Rai stage I–II) with favorable genetics (del 13q) does not require immediate treatment. The "watch-and-wait" approach delays chemotherapy until symptomatic progression or high-risk features emerge, improving quality of life without compromising survival.
CLL Risk Stratification and Treatment Timing
Loading diagram...
Prognostic Markers in CLL
Table
Marker
Prognosis
Median OS
del 13q (sole)
Favorable
>10 years
Normal karyotype
Intermediate
5–8 years
Trisomy 12
Intermediate
5–8 years
del 11q
Adverse
5–8 years
del 17p / TP53 mut
Very adverse
<2 years
High-YieldNEET PG
Rai stage II with del 13q as the sole abnormality is a favorable-risk CLL. Asymptomatic patients do not benefit from early treatment and should be observed.
Clinical Pearl
The "watch-and-wait" approach has been validated in multiple randomized trials (e.g., CLL5 trial) showing no survival disadvantage compared to immediate treatment, while reducing cumulative toxicity.
Indications to Initiate Treatment in CLL
1.
Symptomatic disease: B symptoms (fever, night sweats, weight loss ≥10% in 6 months)
2.
Progressive marrow failure: Hemoglobin <11 g/dL or platelets <100,000/µL due to CLL
3.
Massive/progressive lymphadenopathy or organomegaly causing symptoms
4.
Lymphocyte doubling time <6 months (indicates aggressive biology)
5.
Adverse genetics (del 17p, TP53 mutation, del 11q) even if asymptomatic
Mnemonic
WATCH = Wait for symptoms, Avoid early chemo, Track with labs, Consider genetics, Hold unless high-risk
Why Other Options Are Incorrect
Fludarabine + cyclophosphamide: Chemotherapy is toxic and should not be given to asymptomatic patients with favorable genetics. Reserved for symptomatic or high-risk disease.
Venetoclax monotherapy: BCL2 inhibitor is effective but should not be started without indication; reserved for relapsed/refractory CLL or high-risk disease.
TP53 testing without clinical indication: TP53 mutation testing is not routine in favorable-risk del 13q disease. It is indicated in del 17p, del 11q, or if considering early treatment.
Harrison 21e Ch 105; Robbins 10e Ch 13
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.