## Clinical Diagnosis: Immune Thrombocytopenia (ITP) ### Key Clinical Features **Key Point:** The diagnosis of ITP rests on the triad of (1) thrombocytopenia, (2) normal or increased bone marrow megakaryocytes, and (3) absence of secondary causes. This patient presents with: - Severe thrombocytopenia (18,000/μL) - Mucocutaneous bleeding (epistaxis, gum bleeding, petechiae) - **Normal coagulation studies** (PT and aPTT normal) - **Normocellular bone marrow with normal megakaryocytes** — rules out production defects - **Prolonged bleeding time** — reflects platelet dysfunction or severe thrombocytopenia - **Lifelong history** of heavy menstrual bleeding since menarche — suggests chronic immune-mediated platelet destruction ### Why the Coagulation Studies Are Normal ITP is a **platelet disorder**, not a coagulation factor deficiency. PT and aPTT depend on factors II, V, VII, X (PT) and XII, XI, IX, VIII (aPTT), which are normal in ITP. Bleeding time is prolonged because platelet count is <20,000/μL and/or platelet function is impaired by antibody coating. ### Pathophysiology 1. Autoantibodies (IgG) bind to platelet surface antigens (GPIIb/IIIa, GPIb/IX) 2. Antibody-coated platelets are opsonized and cleared by splenic macrophages 3. Megakaryocytes increase in response (compensatory), but destruction exceeds production 4. Result: **peripheral destruction** with **normal or increased marrow reserves** ### Differential Diagnosis Table | Feature | ITP | DIC | TTP | Bernard–Soulier | |---------|-----|-----|-----|------------------| | **Platelet count** | ↓↓ | ↓↓ | ↓↓ | ↓ (mild–moderate) | | **PT/aPTT** | Normal | ↑↑ | Normal | Normal | | **Fibrinogen** | Normal | ↓↓ | Normal | Normal | | **Schistocytes** | Absent | Present | Present | Absent | | **Bone marrow** | ↑ Megakaryocytes | Normal | Normal | Normal | | **Bleeding time** | ↑ | ↑ | ↑ | ↑↑ (marked) | | **Trigger** | Autoimmune | Sepsis, DKA, malignancy | Shiga toxin, TTP-ADAMTS13 | Congenital | **High-Yield:** In ITP, **coagulation studies are always normal**. If PT or aPTT is prolonged, think DIC or liver disease, not ITP. ### Clinical Pearl The **normocellular bone marrow with increased megakaryocytes** is the gold standard for confirming peripheral destruction rather than bone marrow failure. This finding is pathognomonic for ITP in the presence of thrombocytopenia and normal coagulation studies. ### Management Implications - **First-line:** Corticosteroids (prednisolone 1 mg/kg/day) or IVIG (2 g/kg over 2–5 days) - **Second-line:** Splenectomy (if corticosteroid-responsive), rituximab, TPO-mimetics (eltrombopag, romiplostim) - **Avoid:** NSAIDs, anticoagulants (will worsen bleeding) [cite:Robbins 10e Ch 13] 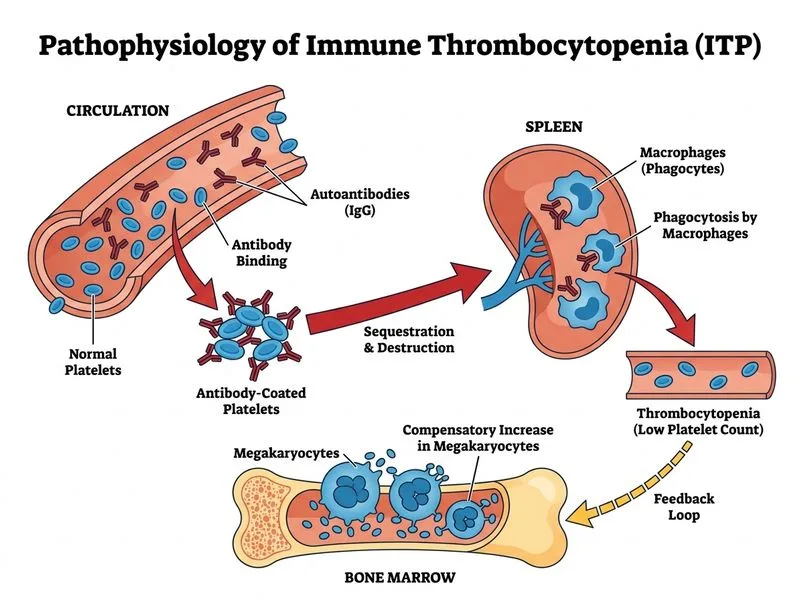
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.