## Coagulopathy in Cirrhosis: Hepatic Synthetic Failure ### Pathophysiology of Cirrhotic Coagulopathy **Key Point:** Cirrhosis causes coagulopathy through **impaired hepatic synthesis** of clotting factors, fibrinogen, and natural anticoagulants (proteins C and S). The liver is the sole site of synthesis for factors II, V, VII, IX, X, XI, XII, and fibrinogen. ### Laboratory Pattern in Cirrhosis | Parameter | Finding | Mechanism | |-----------|---------|----------| | **PT** | ↑↑ (24 sec) | Deficiency of factors II, VII, IX, X (vitamin K-dependent) | | **aPTT** | ↑ (42 sec) | Deficiency of factors II, V, VIII, IX, X, XI, XII | | **Fibrinogen** | ↓ (120 mg/dL) | Impaired hepatic synthesis | | **Platelet count** | ↓ (65,000/μL) | Splenic sequestration (portal hypertension) + bone marrow suppression | | **D-dimer** | ↑ (8.2 μg/mL) | Increased fibrin turnover, renal clearance impairment | | **Factor V** | ↓ | Hepatic synthesis failure (most sensitive indicator) | | **Factor VIII** | Normal or ↑ | Produced by endothelium, not liver; may be elevated due to inflammation | **High-Yield:** The **Factor V:VIII ratio** is a key discriminator: - **Cirrhosis:** Factor V ↓, Factor VIII normal/↑ → ratio <1 ("hepatic synthetic failure") - **DIC:** Both Factor V and VIII ↓ → ratio ~1 ("consumption") ### Why This Patient Has Cirrhotic Coagulopathy 1. **Vitamin K-dependent factors (II, VII, IX, X)** — synthesized exclusively by hepatocytes; cirrhosis → impaired synthesis → prolonged PT 2. **Fibrinogen** — produced by hepatocytes; cirrhosis → low fibrinogen (120 mg/dL) 3. **Factor V** — hepatic synthesis; cirrhosis → deficiency (most sensitive marker of liver synthetic function) 4. **Platelets** — reduced due to splenic sequestration (portal hypertension) and bone marrow suppression 5. **D-dimer elevation** — reflects increased fibrinolysis and impaired renal clearance in cirrhosis ### Pathophysiologic Cascade ```mermaid flowchart TD A[Cirrhosis / Hepatocyte Necrosis]:::outcome --> B[Impaired Hepatic Synthetic Function] B --> C[Deficiency of Factors II, V, VII, IX, X, XI, XII]:::outcome B --> D[Low Fibrinogen]:::outcome B --> E[Reduced Protein C & S]:::outcome A --> F[Portal Hypertension] F --> G[Splenic Sequestration]:::outcome G --> H[Thrombocytopenia]:::outcome C --> I[Prolonged PT/aPTT]:::outcome D --> I H --> I E --> J[Hypercoagulable State Paradoxically]:::outcome J --> K[Portal Vein Thrombosis]:::outcome ``` **Clinical Pearl:** Cirrhotic patients are **paradoxically hypercoagulable** despite prolonged PT/aPTT. This is because: - Anticoagulants (Protein C, Protein S, antithrombin) are also synthesized by the liver and are reduced - Impaired clearance of tissue factor and phosphatidylserine-positive microparticles - Result: **rebalanced hemostasis** — bleeding risk is real but lower than PT/aPTT suggest ### Differential Diagnosis: Why Not the Other Options? **Option 1 — Selective Factor V deficiency with normal Factor VIII:** - This is a **rare congenital disorder**, not a feature of cirrhosis - In cirrhosis, Factor VIII is typically normal or elevated (endothelial source), but Factor V is also low - The pattern here (low Factor V + low Factor VIII + low fibrinogen) is consistent with **global hepatic synthetic failure**, not selective Factor V deficiency **Option 3 — Portal vein thrombosis causing consumption:** - Portal vein thrombosis is a **consequence** of cirrhotic coagulopathy, not the primary mechanism - The coagulopathy precedes and predisposes to thrombosis - DIC-like consumption would show schistocytes and progressive thrombocytopenia; this patient has stable labs **Option 4 — DIC from endotoxemia:** - DIC would show **both Factor V and Factor VIII low** (consumption), not the selective pattern seen here - Fibrinogen would be very low (<50 mg/dL) with active DIC - Schistocytes would be present on blood film - D-dimer elevation alone does not confirm DIC ### Management Implications - **Fresh Frozen Plasma (FFP):** Replaces all vitamin K-dependent factors + fibrinogen (but volume-limited) - **Vitamin K:** Ineffective in cirrhosis (hepatocytes cannot utilize it); only useful if cholestasis/malabsorption - **Platelet transfusion:** For platelet count <50,000/μL or active bleeding - **Recombinant Factor VIIa:** Off-label use for variceal bleeding (bypasses factor deficiencies) - **Variceal bleeding management:** Endoscopic therapy + antibiotics (ceftriaxone) + octreotide [cite:Robbins 10e Ch 13; Harrison 21e Ch 297] 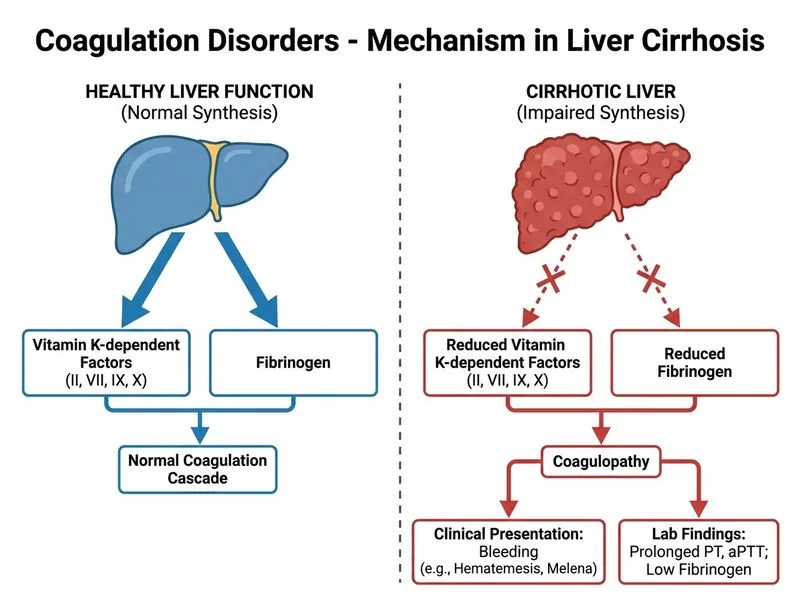
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.