## Acute COPD Exacerbation Management **Key Point:** Acute exacerbations of COPD require a careful balance of oxygenation (avoiding hypoxemia) and ventilation (avoiding CO₂ retention and respiratory acidosis). ## Oxygen Titration Strategy **High-Yield:** Patients with COPD are at risk for **hypercapnic respiratory failure** if given high-concentration oxygen. The target SpO₂ in acute exacerbation is **88–92%** (not 94–98%), which maintains adequate oxygenation while minimizing CO₂ retention. **Clinical Pearl:** Many COPD patients have chronic hypercapnia and rely on hypoxic drive for ventilation. Aggressive oxygen therapy can suppress this drive, worsen CO₂ retention, and precipitate respiratory acidosis. ## Treatment Components | Component | Rationale | |-----------|----------| | **Oxygen (SpO₂ 88–92%)** | Prevents hypoxemia while avoiding CO₂ retention | | **Systemic corticosteroids** | Reduces airway inflammation; given for all moderate-to-severe exacerbations | | **Empirical antibiotics** | Indicated if purulent sputum present; do not wait for culture | | **Bronchodilators** | Increase frequency of SABA ± SAMA | **Mnemonic: ABCDE of COPD Exacerbation** - **A**ntibiotics (if purulent sputum) - **B**ronchodilators (increase frequency) - **C**orticosteroids (systemic) - **D**iuretics (if cor pulmonale) - **E**xygen (target SpO₂ 88–92%) ## Why Empirical Antibiotics? This patient has **purulent sputum and fever**, meeting criteria for bacterial exacerbation. Delaying antibiotics while awaiting culture increases risk of treatment failure and deterioration. Empirical therapy with amoxicillin-clavulanate or fluoroquinolone is standard [cite:GOLD 2023]. 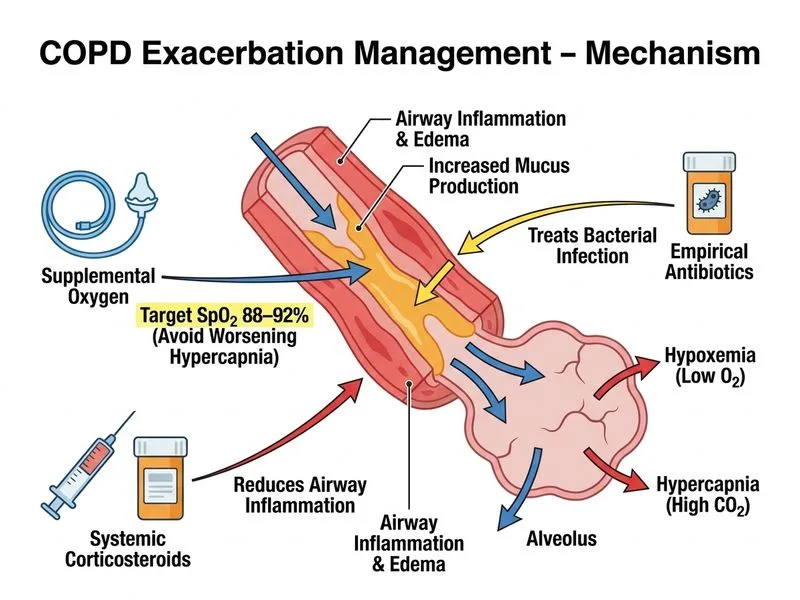
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.