## Acute COPD Exacerbation with Pneumonia: Management Principles **Key Point:** This patient has an acute COPD exacerbation with community-acquired pneumonia (CAP). The critical management principle in COPD is **controlled oxygen therapy** — avoiding hyperoxia that suppresses respiratory drive and worsens CO₂ retention. ### Oxygen Titration in COPD | Scenario | Target SpO₂ | Rationale | |---|---|---| | Stable COPD | 88–92% | Avoid suppressing hypoxic drive; prevent CO₂ retention | | Acute exacerbation without hypercapnia | 88–92% | Same principle; monitor ABG if at risk | | Acute exacerbation with hypercapnia (pH <7.35) | 88–90% | Minimize CO₂ rise; consider NIV | | Acute exacerbation with severe hypoxia (SpO₂ <80%) | Target 88–92% initially, then titrate | Avoid rapid correction | **High-Yield:** The **88–92% target** is the GOLD standard for COPD exacerbations. Overshooting to >94% increases risk of CO₂ narcosis, respiratory acidosis, and need for mechanical ventilation. ### Management Algorithm for This Case ```mermaid flowchart TD A[COPD exacerbation + pneumonia]:::outcome --> B[SpO₂ 88% on RA]:::outcome B --> C{Alert & oriented?}:::decision C -->|Yes| D[Controlled O₂ to 88-92%]:::action C -->|No| E[Consider NIV/intubation]:::urgent D --> F[Nebulized bronchodilators]:::action F --> G[Empirical antibiotics]:::action G --> H[Monitor ABG, respiratory status]:::action H --> I{Improving?}:::decision I -->|Yes| J[Continue therapy]:::action I -->|No| K[Escalate to NIV/intubation]:::urgent ``` ### Why NOT High-Flow Oxygen? 1. **CO₂ retention risk** — COPD patients have blunted CO₂ sensitivity; high FiO₂ removes hypoxic drive 2. **Respiratory acidosis** — SpO₂ >94% often precipitates acute hypercapnic respiratory failure 3. **Intubation risk** — aggressive oxygenation increases need for mechanical ventilation ### Pharmacological Management **Immediate therapy:** - **Nebulized salbutamol ± ipratropium** — rapid bronchodilation - **Systemic corticosteroids** — 30–40 mg prednisolone daily × 5–7 days (reduces exacerbation duration) - **Antibiotics** — empirical coverage for *S. pneumoniae*, *H. influenzae*, *M. catarrhalis*; consider *Pseudomonas* if recent hospitalization **Clinical Pearl:** This patient is **alert and oriented with adequate perfusion** (BP 110/70, HR 110). She does NOT require intubation at presentation. Non-invasive ventilation (NIV) is considered if respiratory acidosis develops (pH <7.30) despite optimal therapy. **Mnemonic:** **COPD + Hypoxia = Controlled O₂** (not aggressive). Target 88–92% SpO₂; monitor ABG; escalate to NIV/intubation only if worsening. 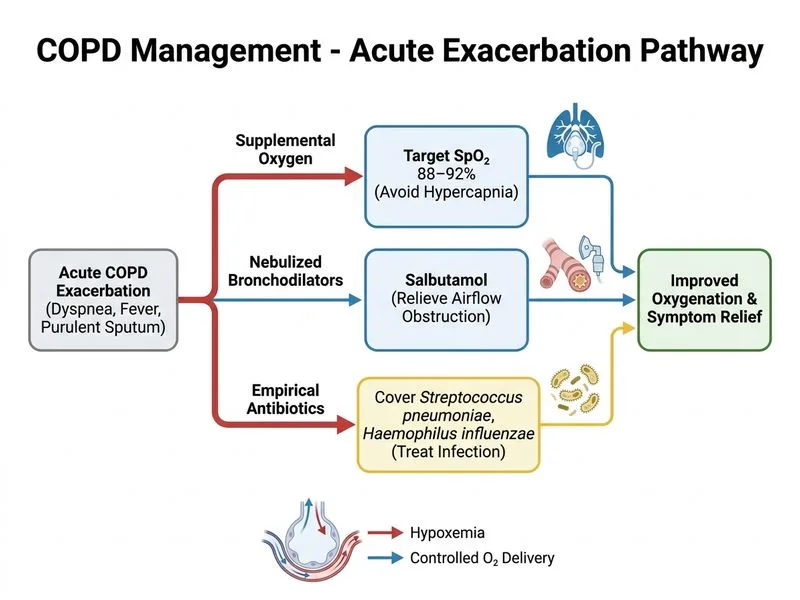
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.