Corneal Ulcer — Bacterial and Fungal MCQ — NEET PG Practice Question | NEETPGAI
Corneal Ulcer — Bacterial and Fungal
medium
eye Ophthalmology
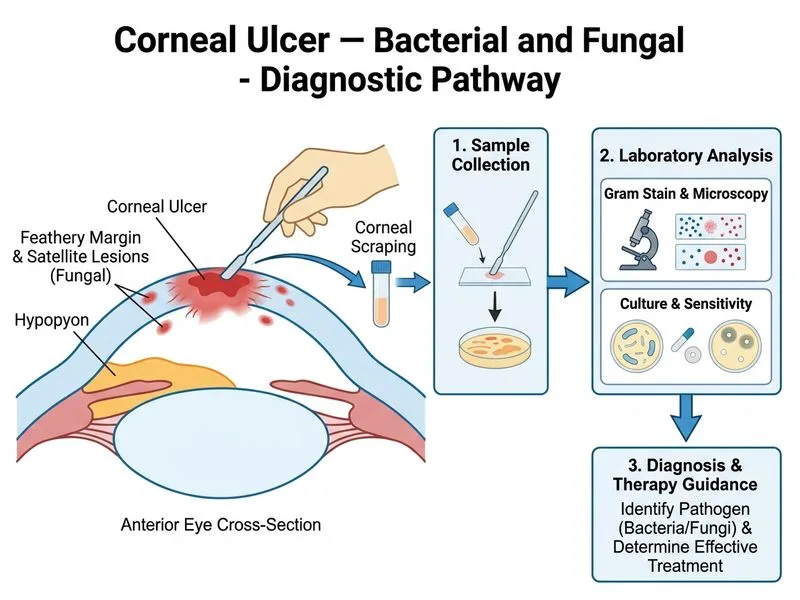
A 52-year-old farmer from rural Maharashtra presents with a 10-day history of painful red eye with photophobia and blurred vision. Slit-lamp examination reveals a central corneal ulcer with raised, infiltrated borders and a hypopyon. The ulcer has a feathery margin and satellite lesions. Which investigation is most appropriate to confirm the diagnosis and guide therapy?
A. Tear film osmolarity measurement
B. Anterior segment optical coherence tomography (AS-OCT)
C. Confocal microscopy of the cornea
D. Corneal scraping for Gram stain, culture, and sensitivity
Explanation
Investigation of Choice for Corneal Ulcer
Key Point
Corneal scraping with Gram stain, culture, and sensitivity is the gold standard for diagnosing bacterial and fungal corneal ulcers and determining antimicrobial susceptibility.
Clinical Presentation Analysis
The patient's presentation is highly suggestive of a fungal corneal ulcer:
Fungal hyphae: KOH mount or Gram stain may show branching filaments
Specimen Collection Protocol
1.
Topical anesthesia (proparacaine 0.5%)
2.
Sterile spatula or Kimura platinum spatula
3.
Scrape the ulcer base and margins (not the surrounding cornea)
4.
Inoculate directly onto:
Blood agar
Chocolate agar
Sabouraud dextrose agar (fungal)
Thioglycollate broth (enrichment)
5.
Prepare smears for Gram stain and KOH mount
Clinical Pearl
In suspected fungal ulcers, always inoculate Sabouraud dextrose agar and request KOH mount; fungal cultures may take 2–4 weeks, so early suspicion guides empiric therapy.