## Clinical Diagnosis: Cushing Disease (ACTH-Secreting Pituitary Microadenoma) ### Key Diagnostic Features **Key Point:** The combination of elevated ACTH (68 pg/mL, within normal-to-high range), positive high-dose dexamethasone suppression (>50% reduction), and MRI evidence of a pituitary adenoma is diagnostic of Cushing disease. ### Dexamethasone Suppression Test Interpretation | Test | Result | Interpretation | |------|--------|----------------| | **Overnight 1 mg DST** | Cortisol 18 µg/dL | Fails to suppress (>1.8) → Cushing syndrome confirmed | | **High-dose 8 mg DST** | Cortisol 8 µg/dL (50% ↓) | **Suppresses >50%** → PITUITARY source | | **ACTH level** | 68 pg/mL | Normal-to-elevated → excludes adrenal adenoma | **High-Yield:** High-dose dexamethasone suppression with >50% reduction in cortisol is the gold standard for distinguishing pituitary Cushing disease from ectopic ACTH syndrome. ### Pathophysiology of Cushing Disease 1. **ACTH-secreting pituitary adenoma** produces excessive ACTH 2. ACTH stimulates adrenal cortex → cortisol overproduction 3. **Negative feedback remains partially intact:** high-dose dexamethasone (8 mg) can suppress the pituitary adenoma 4. Result: >50% reduction in cortisol at 8 mg dexamethasone ### Differential Diagnosis: Pituitary vs. Ectopic ACTH ```mermaid flowchart TD A[Cushing Syndrome Confirmed]:::outcome --> B[ACTH Level?]:::decision B -->|Suppressed <5| C[Adrenal Adenoma]:::outcome B -->|Normal to High| D[High-Dose DST]:::decision D -->|Suppresses >50%| E[ACTH-Secreting Pituitary Adenoma<br/>Cushing Disease]:::action D -->|No Suppression| F[Ectopic ACTH Syndrome]:::urgent E --> G[Pituitary MRI confirms adenoma]:::outcome F --> H[Chest/Abdomen imaging for tumor]:::outcome ``` **Clinical Pearl:** Cushing disease accounts for ~70% of endogenous Cushing syndrome. The 6 mm pituitary lesion is a microadenoma (by definition <10 mm), which is the typical size for ACTH-secreting adenomas. **Mnemonic: High-Dose DST Response = Pituitary Source — PITUITARY SUPPRESSES** - **P**ituitary adenoma → suppresses at high dose (>50% ↓) - **I**s the diagnosis when imaging shows adenoma - **T**ypical ACTH level: normal to mildly elevated - **U**nder negative feedback control - **I**nhibited by high-dose dexamethasone - **T**est: 8 mg DST shows >50% suppression - **A**CTH-secreting microadenoma - **R**esult: Cushing disease - **Y**ield: Best prognosis with transsphenoidal surgery ### Imaging Findings - **Pituitary MRI:** 6 mm hypodense lesion in anterior pituitary consistent with microadenoma - **Adrenal imaging:** Would show bilateral adrenal hyperplasia (not described here, but expected in Cushing disease) ### Next Steps in Management 1. **Transsphenoidal pituitary surgery** — first-line definitive treatment 2. **Bilateral inferior petrosal sinus sampling (IPSS)** — if MRI inconclusive (not needed here given clear findings) 3. **Post-operative cortisol monitoring** — confirm remission 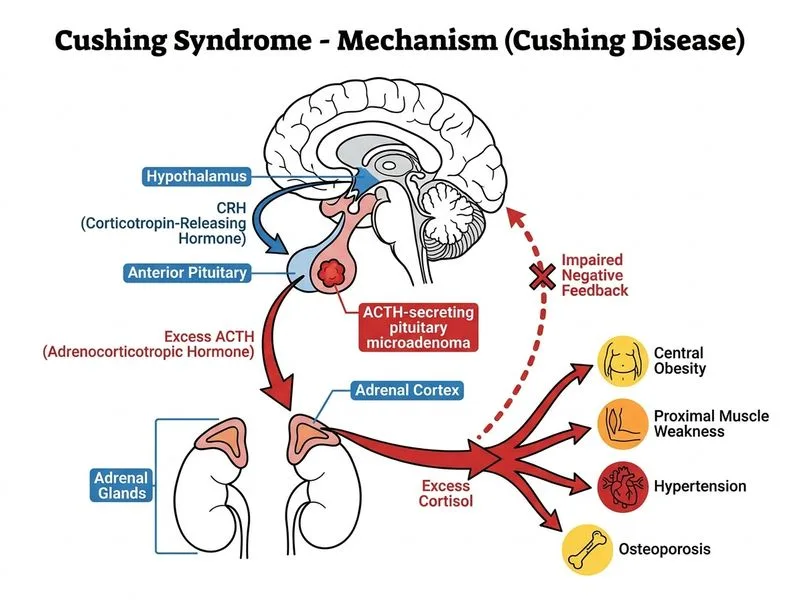
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.