## Diagnosis of Primary Adrenal Cushing Syndrome **Key Point:** The combination of elevated 24-hour UFC with **suppressed ACTH** (8 pg/mL, well below normal) is pathognomonic for **primary adrenal disease** (adenoma or carcinoma). The low ACTH indicates the pituitary is appropriately suppressed by excess cortisol, confirming the adrenal gland is the autonomous source. ### Differential Diagnosis by ACTH Level | Diagnosis | ACTH Level | UFC | LDDST | HDDST | Imaging | |-----------|-----------|-----|-------|-------|----------| | **Cushing Disease** | Normal/↑ (10–50) | ↑↑ | No supp. | **Suppresses** | Pituitary adenoma | | **Ectopic ACTH** | ↑↑ (>100) | ↑↑↑ | No supp. | No supp. | Lung/GI tumor | | **Primary Adrenal** | **↓ (<5)** | ↑↑ | No supp. | No supp. | Adrenal mass | **High-Yield:** ACTH <5 pg/mL in the presence of elevated cortisol/UFC is diagnostic of primary adrenal disease. This patient's ACTH of 8 pg/mL (suppressed) with UFC 180 µg/day confirms adrenal source. ### Distinguishing Adrenal Adenoma from Carcinoma | Feature | Adenoma | Carcinoma | |---------|---------|----------| | **Age** | 40–60 years | 40–50 years (can overlap) | | **Presentation** | Insidious, Cushing features | Rapid, severe, ± virilization | | **Tumor size** | <4 cm (usually) | >4 cm, often >6 cm | | **Imaging (CT)** | Homogeneous, low density, <10 HU | Heterogeneous, high density, >10 HU, necrosis | | **Hormonal excess** | Cortisol only | Cortisol + androgens (virilization) | | **Prognosis** | Excellent post-surgery | Poor; 5-year survival ~30% | **Clinical Pearl:** This patient presents with classic Cushing features (2-year history, central obesity, purple striae, proximal myopathy, hypertension, new-onset diabetes) and suppressed ACTH. The gradual onset and absence of virilization favor **adrenal adenoma** over carcinoma. Definitive diagnosis requires adrenal CT/MRI to assess tumor size, density, and imaging characteristics. ### Why ACTH Suppression Occurs When the adrenal gland autonomously secretes excess cortisol, negative feedback at the pituitary and hypothalamus suppresses CRH and ACTH release. The pituitary is functioning normally but is "turned off" by the high cortisol. This is in contrast to Cushing disease, where the pituitary adenoma is insensitive to feedback and continues to produce ACTH despite elevated cortisol. 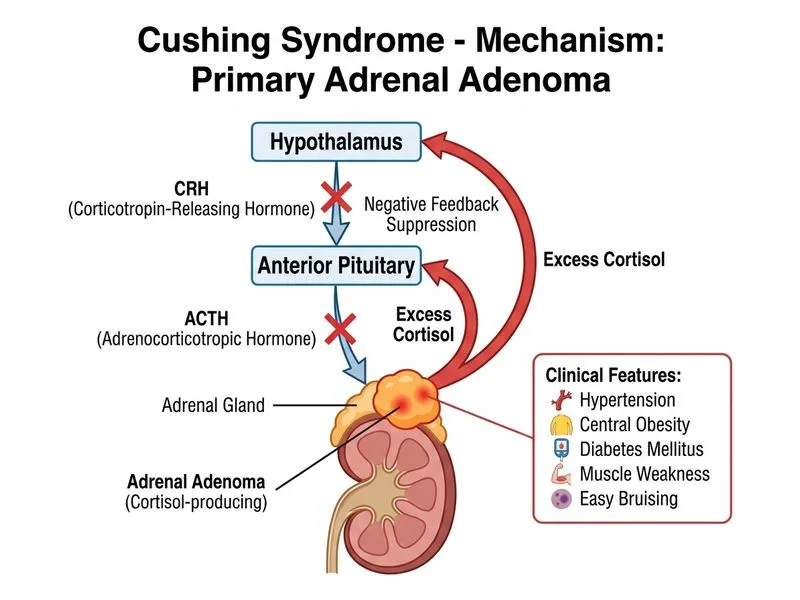
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.