A 38-year-old woman with acute promyelocytic leukemia (APL) presents to the ICU with severe bleeding from multiple sites (gums, GI tract, vagina) and petechiae. Laboratory investigations show: PT 18 sec (control 12), aPTT 45 sec (control 35), fibrinogen 85 mg/dL, D-dimer >10 µg/mL (normal <0.5), and platelet count 22,000/µL. Peripheral blood shows abnormal promyelocytes with Auer rods. What is the most appropriate immediate next step in management?
A. Transfuse packed red cells and platelets only, defer specific treatment until coagulation studies normalize
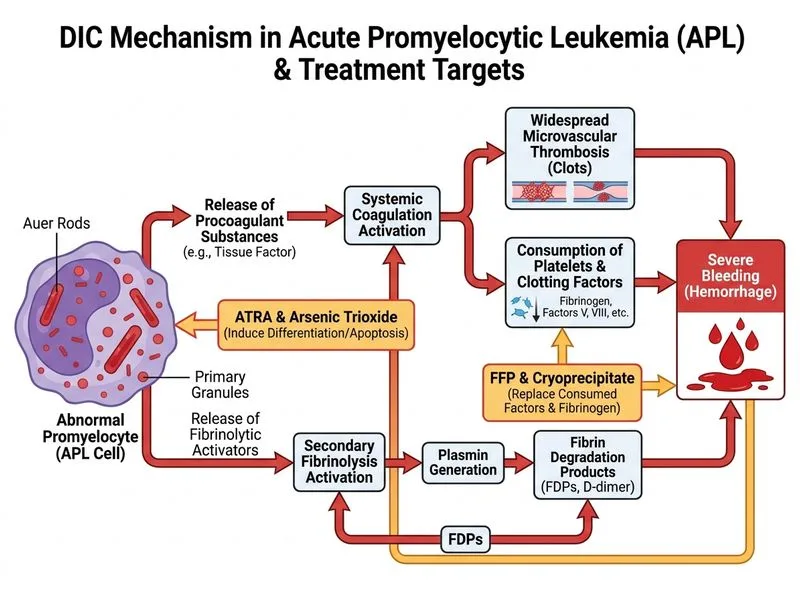
B. Start fresh frozen plasma and cryoprecipitate transfusion along with all-trans retinoic acid (ATRA) and arsenic trioxide
C. Perform bone marrow biopsy to confirm APL diagnosis before initiating any treatment
Start high-dose heparin to prevent further thrombus formation
D.
Explanation
Clinical Context: DIC in APL
This patient has disseminated intravascular coagulation (DIC) secondary to acute promyelocytic leukemia (APL), a medical emergency with a mortality rate >80% if untreated.
Key Diagnostic Findings
High-YieldNEET PG
APL is the most common cause of DIC among hematologic malignancies due to release of tissue factor and cancer procoagulant from abnormal promyelocytes.
Table
Finding
Interpretation
PT/aPTT prolonged
Consumption of clotting factors
Fibrinogen 85 mg/dL
Severe hypofibrinogenemia (normal >100)
D-dimer markedly elevated
Massive fibrin formation and breakdown
Thrombocytopenia + bleeding
Platelet consumption
Auer rods on blood smear
Pathognomonic for APL
Management Algorithm
Loading diagram...
Why This Answer Is Correct
Key Point
The immediate management of DIC-APL requires simultaneous correction of coagulopathy AND initiation of definitive APL therapy.
1.
FFP + Cryoprecipitate: Replace consumed clotting factors and fibrinogen to stop active bleeding. Cryoprecipitate is preferred for fibrinogen repletion (10 units raises fibrinogen ~50 mg/dL).
2.
ATRA + Arsenic trioxide: These are the definitive treatments for APL. ATRA induces differentiation of leukemic promyelocytes, reducing release of procoagulant substances and allowing DIC to resolve. Arsenic trioxide is the backbone of modern APL therapy.
3.
Timing is critical: Delaying APL-specific therapy worsens DIC; early initiation leads to rapid resolution of coagulopathy as leukemic burden decreases.
Clinical Pearl
ATRA is contraindicated in pregnancy (teratogenic) but is safe in this non-pregnant adult. The combination of ATRA + arsenic trioxide achieves cure rates >90% in APL.
High-YieldNEET PG
DIC in APL is self-limited — it resolves with successful treatment of the underlying leukemia. Do NOT use anticoagulation (heparin) as first-line; it worsens bleeding.
Robbins 10e Ch 13
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.