## Clinical Diagnosis: DIC Secondary to Sepsis ### Presentation Analysis This patient presents with a classic triad for DIC: 1. **Trigger:** Sepsis from retained products of conception (unsafe abortion) 2. **Hemodynamic instability:** Hypotension and tachycardia indicating shock 3. **Multisystem involvement:** Fever, bleeding, organ hypoperfusion ### Laboratory Findings Consistent with DIC | Parameter | Finding | Interpretation | |-----------|---------|----------------| | Platelet count | 45,000/µL | Moderate thrombocytopenia from consumption | | PT/aPTT | Both prolonged | Consumption of clotting factors | | Fibrinogen | 85 mg/dL (low) | Consumption and ongoing proteolysis | | D-dimer | >10 µg/mL (markedly elevated) | Massive thrombin generation and fibrinolysis | | Hb | 7.2 g/dL | Bleeding + hemolysis from microangiopathy | **Key Point:** The combination of **thrombocytopenia + coagulopathy + fibrinogen consumption + elevated D-dimer** in the setting of a known trigger (sepsis) is pathognomonic for DIC. ### Pathophysiology of DIC in This Case ```mermaid flowchart TD A[Unsafe abortion with retained POC]:::outcome --> B[Bacterial contamination & tissue factor release]:::action B --> C[Systemic inflammation & endothelial injury]:::action C --> D[Uncontrolled thrombin generation]:::urgent D --> E[Platelet consumption & fibrin deposition]:::action D --> F[Fibrinolysis activation]:::action E --> G[Microangiopathic hemolytic anemia]:::outcome E --> H[Thrombocytopenia]:::outcome F --> I[Fibrinogen depletion]:::outcome F --> J[Elevated D-dimer/FDP]:::outcome H --> K[Bleeding manifestations]:::urgent G --> L[Organ dysfunction]:::urgent ``` ### DIC Scoring (ISTH Criteria) This patient meets criteria for **overt DIC**: - Platelet count drop: 45,000/µL (≥2 points) - D-dimer/FDP elevation: markedly elevated (≥3 points) - PT prolongation: 18 sec (≥1 point) - Fibrinogen: 85 mg/dL (≥1 point) - **Total score ≥5 = compatible with overt DIC** **High-Yield:** DIC is a **consumption coagulopathy** — all clotting factors and platelets are being used up faster than they can be produced, leading to paradoxical bleeding despite hypercoagulability. **Clinical Pearl:** The presence of **sepsis + shock + thrombocytopenia + coagulopathy** is the clinical pearl triad for DIC. Always look for the underlying trigger (infection, trauma, malignancy, obstetric emergency). ### Management Implications 1. Aggressive source control (evacuation of retained POC) 2. Broad-spectrum antibiotics 3. Supportive care with FFP, platelets, cryoprecipitate 4. Treatment of underlying sepsis **Warning:** Do NOT give heparin in acute DIC with active bleeding — it worsens hemorrhage. Anticoagulation is reserved for chronic DIC or thrombotic-predominant DIC. 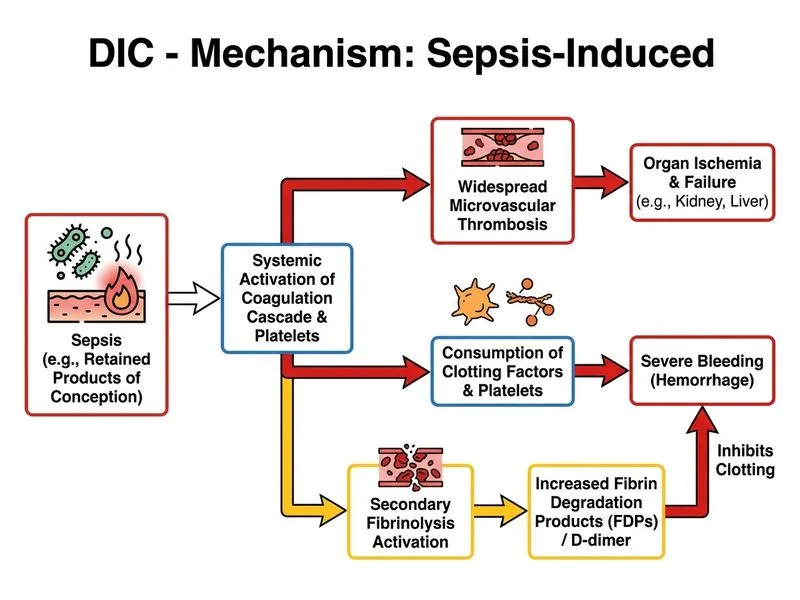
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.