## Management of DIC in Acute Promyelocytic Leukemia (APL) ### Clinical Context: APL-Specific DIC This patient has **acute promyelocytic leukemia (APL, AML-M3)** with **DIC**, a medical emergency. APL is unique because: - It is the **most common cause of DIC among hematologic malignancies** - Leukemic promyelocytes release **tissue factor (TF) and cancer procoagulant** into circulation - DIC develops in ~80% of APL cases and is a leading cause of early death - **Paradoxically, APL is also the most curable AML subtype** when managed correctly ### Laboratory Confirmation of DIC in APL | Finding | This Patient | Interpretation | |---------|--------------|----------------| | Platelet count | 18,000/µL | Severe thrombocytopenia from consumption | | PT/aPTT | Both prolonged | Factor consumption | | Fibrinogen | 95 mg/dL | Hypofibrinogenemia from consumption | | D-dimer | 8.5 µg/mL | Massive fibrinolysis | | Auer rods on smear | Present | Diagnostic for AML; in APL context = t(15;17) | | Hemodynamic instability | BP 92/58, HR 112 | Shock from bleeding and cytokine release | **Key Point:** The combination of **AML-M3 morphology (Auer rods) + severe DIC + bleeding** is pathognomonic for APL-associated DIC. ### Why ATRA + ATO is the Correct Answer ```mermaid flowchart TD A[APL diagnosis confirmed]:::outcome --> B[DIC present with bleeding]:::urgent B --> C{Immediate management?}:::decision C -->|Supportive only| D[Continued bleeding & death]:::urgent C -->|ATRA + ATO| E[Differentiation of blasts]:::action E --> F[Reduction of TF/cancer procoagulant]:::action F --> G[Resolution of DIC within 1-2 weeks]:::outcome G --> H[Cure of APL achieved]:::outcome C -->|Heparin| I[Worsens bleeding]:::urgent C -->|Splenectomy| J[Irrelevant to pathophysiology]:::urgent ``` ### Mechanism: Why ATRA/ATO Works in APL-DIC 1. **ATRA (All-Trans Retinoic Acid)** - Induces differentiation of leukemic promyelocytes → mature neutrophils - Mature cells do NOT release tissue factor or cancer procoagulant - Reduces the **source** of DIC trigger - DIC resolves as promyelocytes differentiate (typically 1–2 weeks) 2. **Arsenic Trioxide (ATO)** - Induces apoptosis of leukemic cells - Synergistic with ATRA - Reduces leukemic burden and TF release 3. **Supportive Transfusions (FFP + Cryoprecipitate)** - **FFP:** Replaces consumed clotting factors (II, V, VII, X, fibrinogen) - **Cryoprecipitate:** Replaces fibrinogen (each unit raises fibrinogen by ~10 mg/dL; target >100 mg/dL) - **Platelet transfusions:** Maintain platelet count >20,000/µL (higher threshold in APL due to bleeding risk) - These are **bridge therapy** while ATRA/ATO takes effect **High-Yield:** The key insight is that **treating the underlying APL (with ATRA/ATO) is the definitive treatment for APL-DIC**. Simply transfusing blood products without addressing the source of TF release will fail. **Clinical Pearl:** APL-DIC is a **medical emergency** but also a **medical miracle** — it is one of the few cancers where DIC is a sign of curability. With ATRA/ATO + supportive care, >90% of APL patients achieve complete remission and cure. ### Why NOT the Other Options **Heparin (Option 3):** - **Absolutely contraindicated** in APL-DIC with active bleeding - Heparin blocks thrombin but does NOT address the underlying TF release - Worsens hemorrhage and increases mortality - Reserved only for chronic DIC or thrombotic-predominant DIC (rare in APL) **Splenectomy (Option 4):** - Spleen is NOT the source of TF in APL - Splenectomy does not reduce promyelocyte-derived TF - Irrelevant to APL pathophysiology - Unnecessary surgical risk in a critically ill patient **Platelet Transfusion Alone (Option 2):** - Transfused platelets are immediately consumed by ongoing DIC - Does NOT address the source of coagulation activation (TF from promyelocytes) - Continuation of standard chemotherapy (e.g., daunorubicin + cytarabine) would worsen DIC and bleeding - ATRA/ATO, not standard chemotherapy, is the induction regimen for APL 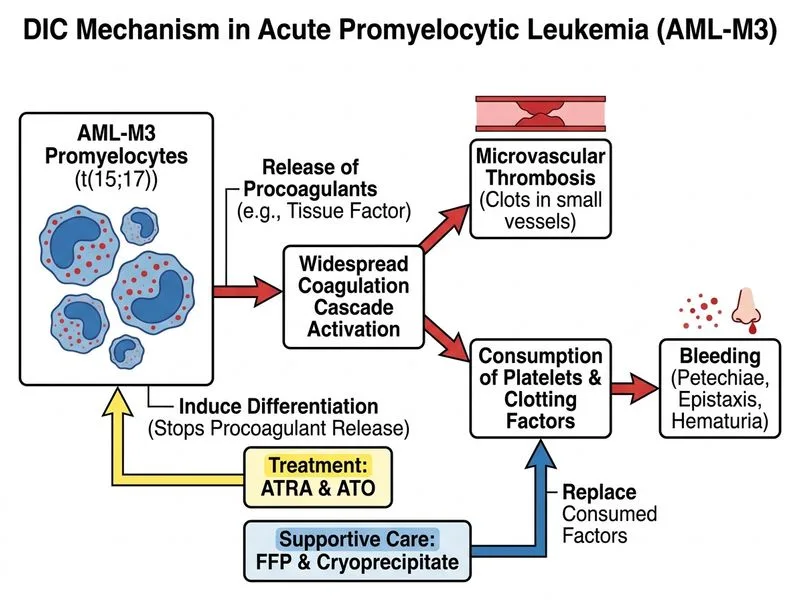
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.