## Difficult Airway Management: Failed Intubation Protocol ### Clinical Context This patient presents with a **predicted difficult airway** (known Cormack–Lehane Grade 3 history) and has now had **two failed intubation attempts** with declining oxygenation (SpO₂ 88%). The airway team is in the **"Can't Intubate, Can Ventilate"** scenario. ### Why Video Laryngoscopy Is Correct **Key Point:** According to the Difficult Airway Society (DAS) guidelines and ASA difficult airway algorithm, after failed conventional laryngoscopy in a patient who can be ventilated, the next escalation step is to use an **alternative intubation device** — specifically a video laryngoscope (VL) — before resorting to emergency surgical airway. - Video laryngoscopes improve the view of the glottis by 1–2 Cormack–Lehane grades in ~80% of difficult cases - They bypass the line-of-sight limitation of direct laryngoscopy - The patient is currently oxygenating adequately with bag-mask ventilation (SpO₂ 88% is concerning but not yet critical; time remains for a controlled attempt) - This is a **controlled, elective scenario**, not an emergency where cricothyrotomy would be the immediate choice ### Algorithm Sequence 1. **First-line:** Direct laryngoscopy (attempted × 2) ✓ Failed 2. **Second-line:** Alternative device (VL) ← **Current step** 3. **Third-line:** Surgical airway (cricothyrotomy/tracheostomy) if VL fails and oxygenation deteriorates **High-Yield:** In the "Can't Intubate, Can Ventilate" scenario, **do not jump to cricothyrotomy prematurely**. Video laryngoscopy has a high success rate and preserves the patient's airway anatomy for future anesthetics. ### Citation **Difficult Airway Society Guidelines (2015) / ASA Difficult Airway Algorithm; Latto et al. Anaesthesia 2015; Apfelbaum et al. Anesthesiology 2013** 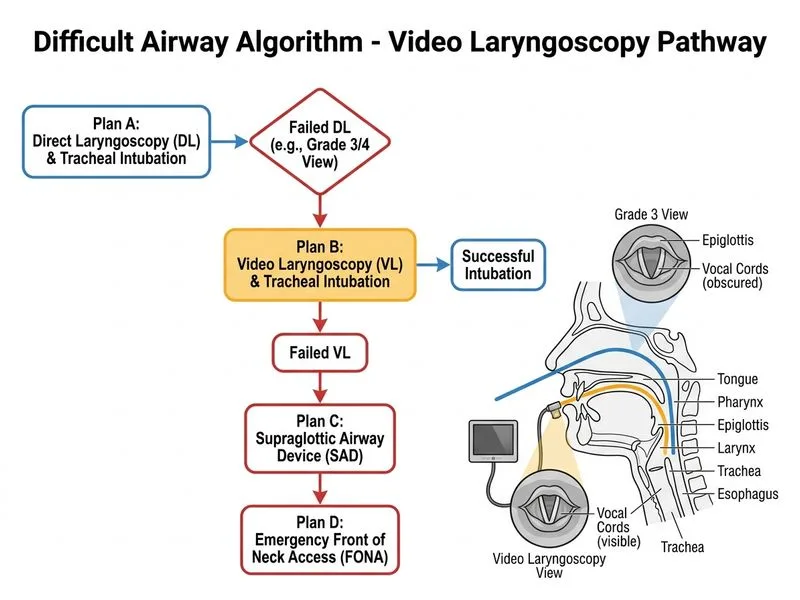
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.