## Difficult Airway Management in the Operating Room This scenario describes a **cannot intubate, can ventilate (CICV)** situation—a critical airway emergency requiring adherence to the Difficult Airway Society (DAS) and ASA guidelines. ### Why Option 1 (Cricothyrotomy) is Incorrect: - Cricothyrotomy is reserved for **cannot intubate, cannot ventilate (CICNV)** scenarios. - In this case, bag-mask ventilation is **adequate**, meaning oxygenation can be maintained. - Performing cricothyrotomy when ventilation is possible is unnecessarily invasive and violates the stepwise escalation principle. ### Why Option 2 is Correct: **This follows the DAS Difficult Airway Algorithm:** 1. **Call for help** — activate the difficult airway team. 2. **Position supine** — optimize head and neck alignment (ramped position, sniffing position). 3. **Video laryngoscopy (VL)** — VL has a higher first-pass success rate (60–80%) compared to direct laryngoscopy (30–40%) in difficult airways. 4. **Reduce stylet curve** — decreases the risk of esophageal intubation and trauma in restricted views. 5. **Alter blade angle** — allows visualization of vocal cords in anterior larynx. 6. **Maintain oxygenation** — continue bag-mask ventilation between attempts; SpO₂ 88% is still acceptable for one more coordinated attempt. **Key Point:** In CICV, the goal is to **maintain oxygenation while securing the airway** using escalated techniques (VL, bougie, different blades) before considering surgical airway. ### Why Option 3 (Abort and Reschedule) is Incorrect: - While awake fiberoptic intubation is **gold standard** for predicted difficult airways, it should have been planned **preoperatively** given the obvious risk factors (Mallampati III, limited neck extension, OSA, obesity). - Aborting now wastes time and exposes the patient to repeated anesthesia induction. - In the OR with adequate ventilation, a coordinated attempt with VL is safer and more efficient than waking the patient and rescheduling. ### Why Option 4 (Continue with Larger Tube and More Sedation) is Incorrect: - **Larger tubes** do not improve visualization; they may worsen trauma and increase aspiration risk. - **Increased sedation** in an already-intubated patient risks apnea and worsening hypoxemia. - This represents **continued blind attempts**, which violates the principle of escalation and increases morbidity. ## Clinical Pearl: **The Difficult Airway Society Algorithm emphasizes:** - Plan A (DL) → Plan B (VL, bougie) → Plan C (LMA, FONA) → Plan D (Surgical airway). - CICV = use Plans B and C; CICNV = Plan D (cricothyrotomy/tracheostomy). ## High-Yield Mnemonic: **"STOP and CALL"** - **S**witch technique (VL, bougie) - **T**ake time (do not rush) - **O**xygenate between attempts - **P**osition optimize - **C**all for help - **A**lternate blade/angle - **L**MA/surgical airway if needed - **L**isten to team communication 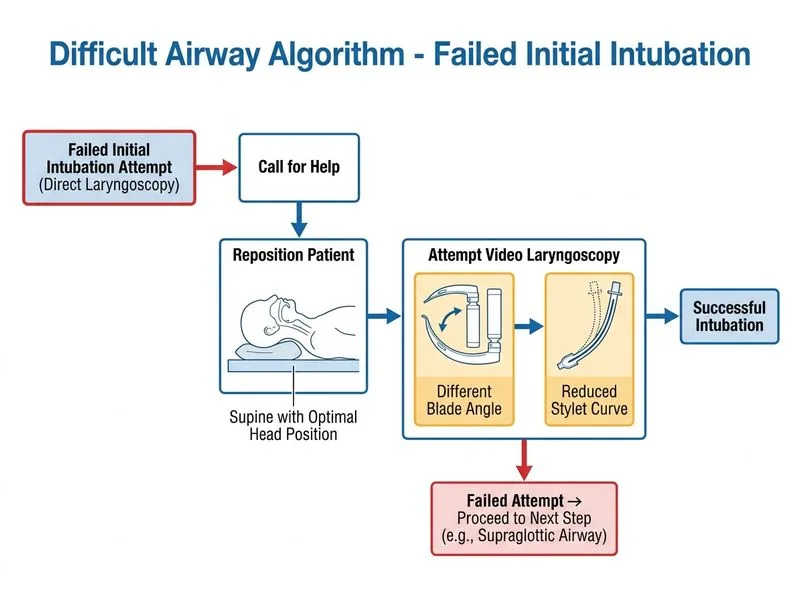
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.