## Difficult Airway Management in the Paralyzed Patient This scenario represents a **cannot intubate, can oxygenate (CICO)** situation with a predicted difficult airway that was not managed preoperatively. ### Key Point: When faced with Grade 3 view and failed intubation attempts in a paralyzed patient with adequate oxygenation (SpO₂ 88% is still acceptable for a brief period), the next step is **escalation of intubation technique** rather than immediate surgical airway or wake-up. ### Rationale for Correct Answer (Option 1 – Video Laryngoscope with Bougie): - **Video laryngoscopes** (Glidescope, C-MAC) provide superior visualization compared to direct laryngoscopy, particularly in Grade 3 views - **Bougie use** increases first-pass success rate in difficult intubation (80–90% success with bougie vs. 50% without) - **Apneic oxygenation** (high-flow nasal oxygen at 15 L/min) extends safe apnea time to 8–10 minutes in pre-oxygenated patients - This approach preserves the option of surgical airway if video laryngoscopy also fails - Current **Difficult Airway Society (DAS) 2015 guidelines** recommend video laryngoscopy as the next escalation step after failed direct laryngoscopy in a paralyzed patient ### Why Other Options Are Suboptimal: - **Cricothyrotomy (Option 0):** Indicated only when intubation AND ventilation fail (CICO situation with cannot oxygenate). Here, oxygenation is still adequate; premature surgical airway increases morbidity. - **Abort and reschedule (Option 2):** Abandoning the case after induction and paralysis risks aspiration, hypoxemia during emergence, and loss of airway control. Only appropriate if intubation remains impossible after all escalation attempts. - **Blind nasal intubation (Option 3):** Contraindicated in a paralyzed patient; also carries risk of epistaxis and tube malposition. Nasal intubation is a technique for awake patients or those with preserved spontaneous ventilation. ### Clinical Pearl: **Escalation ladder in paralyzed difficult intubation:** 1. Direct laryngoscopy (failed) 2. **Video laryngoscopy ± bougie** (next step) 3. Fiberoptic bronchoscope (if video fails) 4. Surgical airway (last resort if all fail and cannot oxygenate) ### High-Yield: In a **CICO-can oxygenate** scenario, always attempt non-surgical escalation (video laryngoscope, bougie, fiberoptic) before resorting to cricothyrotomy. 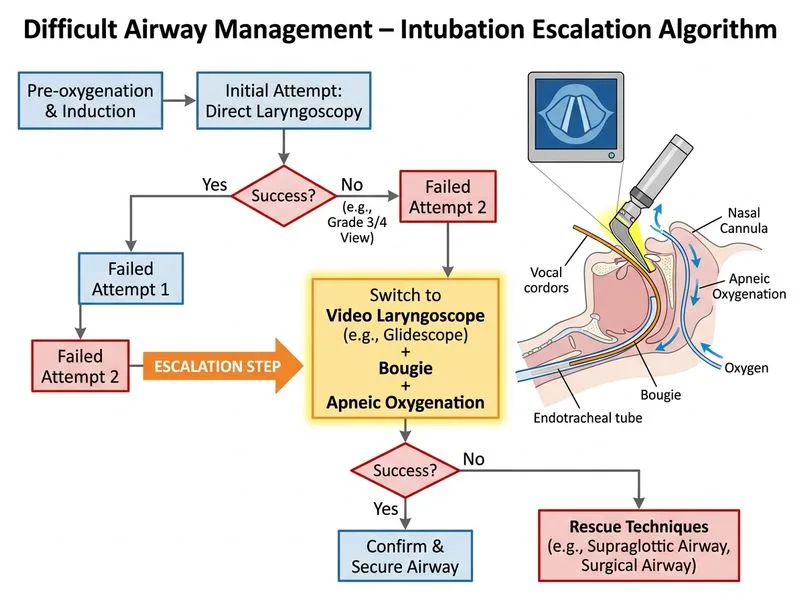
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.