A 58-year-old man from Delhi presents to the emergency department with acute onset chest pain radiating to the left arm for 2 hours. He is diaphoretic and anxious. Vital signs: BP 128/82 mmHg, HR 92 bpm, RR 18/min. On examination, he has no murmurs or crackles. His ECG shows ST-segment elevation in leads II, III, and aVF with reciprocal ST depression in leads I and aVL. Troponin I is elevated at 2.8 ng/mL. What is the most likely diagnosis?
A. Unstable angina with non-ST elevation
B. Left circumflex artery occlusion
C. Inferior wall ST-elevation myocardial infarction
D. Anterior wall ST-elevation myocardial infarction
Explanation
Clinical Presentation and ECG Correlation
Key Point
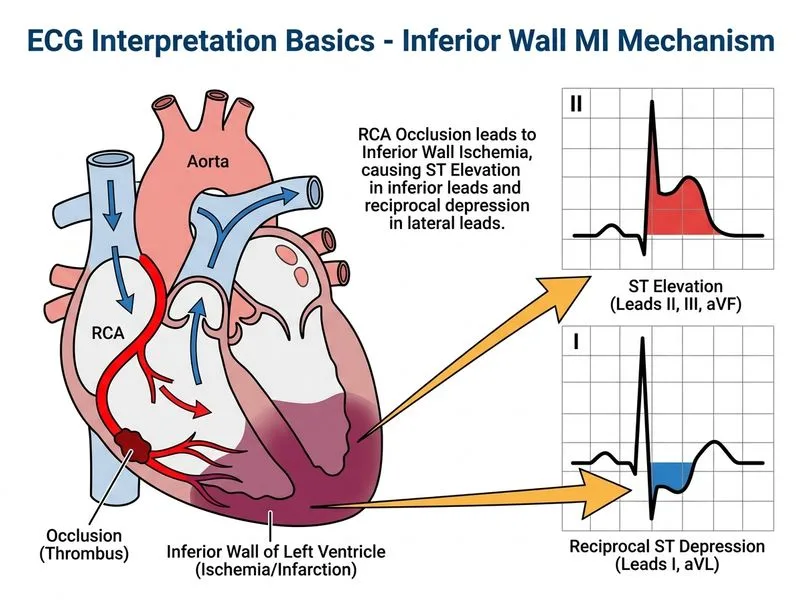
ST-segment elevation in the inferior leads (II, III, aVF) with reciprocal ST depression in the lateral leads (I, aVL) is pathognomonic for inferior wall STEMI.
Anatomical Basis
The inferior wall of the left ventricle is supplied by the right coronary artery (RCA) in approximately 80% of the population. Acute occlusion of the RCA causes:
ST elevation in leads II, III, and aVF
Reciprocal ST depression in leads I and aVL
Possible involvement of the right ventricle (check lead V4R)
ECG Findings in Inferior STEMI
Table
Feature
Inferior STEMI
Anterior STEMI
ST elevation leads
II, III, aVF
V1–V4 (anterior) or V1–V6 (extensive)
Reciprocal changes
I, aVL
None or minimal
Coronary artery
RCA (80%), LCx (20%)
LAD
Complications
RV infarction, bradycardia, AV block
Cardiogenic shock, heart failure
Clinical Pearl
Inferior STEMI frequently presents with bradycardia and hypotension due to increased vagal tone and possible RV involvement. Always check lead V4R for right ventricular infarction, which contraindicates nitrates and requires fluid resuscitation.