This patient presents with acute ST-elevation myocardial infarction (STEMI) of the inferior wall (ST elevation in II, III, aVF with reciprocal changes in I, aVL).
Inferior STEMI typically results from right coronary artery (RCA) occlusion (85% of cases). The ST elevation indicates acute transmural myocardial necrosis with ongoing myocardial injury — time-sensitive intervention is critical to salvage viable myocardium.
Primary PCI is the gold standard for STEMI management when performed within 120 minutes of first medical contact (FMC). In this case, the patient is within the therapeutic window and dual antiplatelet therapy (aspirin + P2Y₁₂ inhibitor) must be initiated immediately before PCI.
| Intervention | Timing | Evidence |
|---|---|---|
| Dual antiplatelet therapy | Immediately (pre-PCI) | Reduces stent thrombosis & mortality |
| Primary PCI | Within 90 min of FMC (120 min acceptable) | Superior to fibrinolysis; reduces reinfarction |
| Fibrinolysis | If PCI unavailable; within 30 min of FMC | Backup strategy; higher reinfarction risk |
Inferior STEMI with RV involvement (look for ST elevation in V4R) requires careful fluid management — avoid aggressive diuresis as RV infarction is preload-dependent. However, this does not change the acute reperfusion strategy.
Troponin and repeat ECG are diagnostic tools, not therapeutic interventions — in acute STEMI, diagnosis is already established by ECG; time must not be wasted on confirmatory testing. The mantra is "time is myocardium."
Harrison 21e Ch 297
Loading illustration…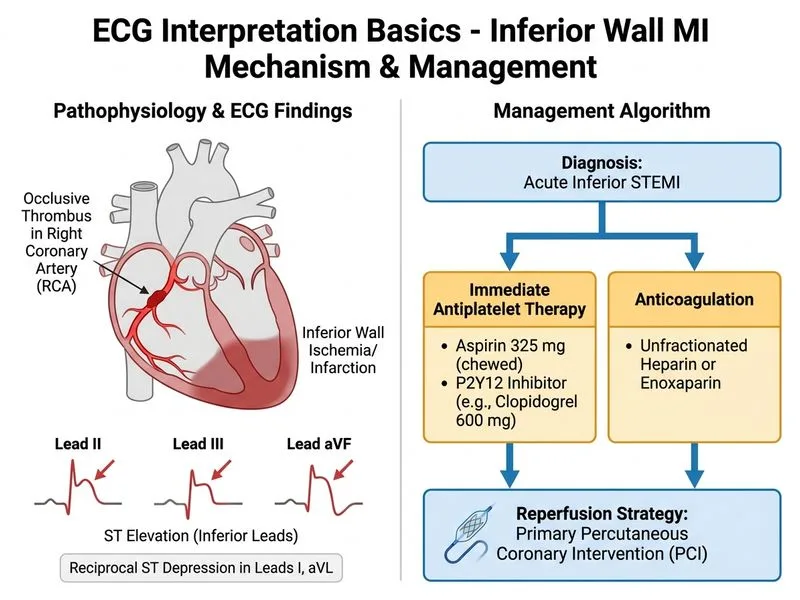
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →