## Clinical Diagnosis: Acute Inferior Wall MI ### ECG Localization by Leads | Wall | ST Elevation Leads | Reciprocal Changes | Coronary Artery | |------|-------------------|-------------------|------------------| | **Inferior** | II, III, aVF | I, aVL | RCA (90%) or LCx (10%) | | Anterior | V1–V4 | II, III, aVF | LAD | | Lateral | I, aVL, V5–V6 | II, III, aVF | LCx | | Posterior | Tall R in V1–V2, ST ↓ in V1–V2 | — | RCA or LCx | **Key Point:** ST elevation in the inferior leads (II, III, aVF) with reciprocal ST depression in the high lateral leads (I, aVL) is pathognomonic for acute inferior wall MI. **High-Yield:** The right coronary artery (RCA) supplies the inferior wall in ~90% of the population; the left circumflex (LCx) in ~10%. Always check for right ventricular involvement in inferior MI by obtaining a right-sided ECG (V4R). **Clinical Pearl:** Inferior MI patients are at risk for: - Bradycardia and AV block (due to RCA supply to the AV node) - Right ventricular infarction (if RCA occlusion is proximal) - Cardiogenic shock (especially with RV involvement) **Warning:** Do NOT give IV nitrates or diuretics in inferior MI with suspected RV involvement—these patients are preload-dependent and may develop severe hypotension. ### Why This Patient Has Inferior MI 1. **ST elevation in II, III, aVF** — the anatomical signature of inferior wall ischemia 2. **Reciprocal ST depression in I, aVL** — confirms inferior localization 3. **Elevated troponin** — confirms myocardial necrosis 4. **Clinical presentation** — acute substernal chest pain with diaphoresis and autonomic symptoms 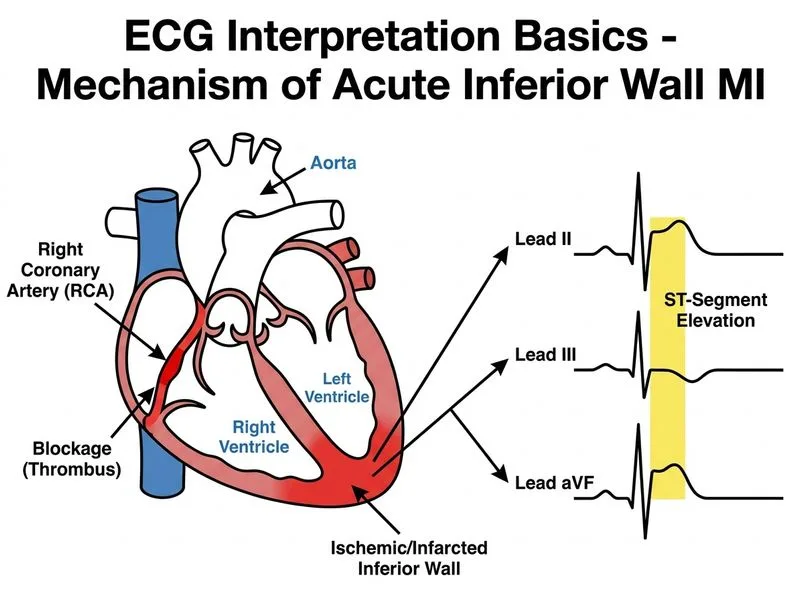
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.