Fracture Classification — Types and Patterns MCQ — NEET PG Practice Question | NEETPGAI
Fracture Classification — Types and Patterns
medium
bone Orthopedics
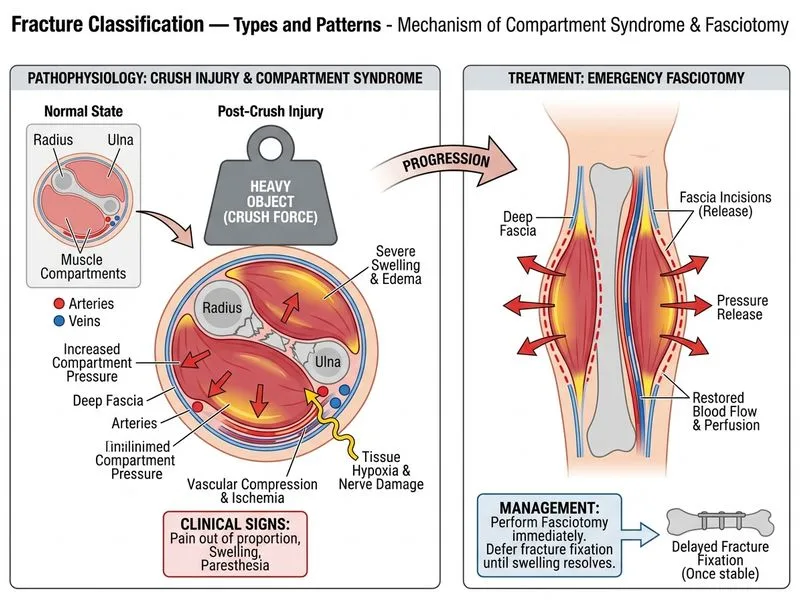
A 32-year-old male labourer presents to the emergency department with a crush injury to his right forearm sustained 6 hours ago when a heavy metal beam fell on him. Clinical examination reveals severe soft tissue swelling, crepitus, and compartment syndrome is suspected. Plain radiographs show a comminuted fracture of the radius and ulna with multiple bone fragments. What is the most appropriate immediate next step in management?
A. Arrange for urgent MRI to assess soft tissue injury extent
B. Apply a below-elbow plaster cast after manual reduction
C. Administer intravenous antibiotics and observe for 24 hours
D. Perform emergency fasciotomy and defer fracture fixation until soft tissue swelling resolves
Explanation
Clinical Context
This is a crush injury with suspected compartment syndrome — a surgical emergency requiring immediate decompression to prevent tissue necrosis, rhabdomyolysis, and renal failure.
Why Emergency Fasciotomy is the Correct Answer
Key Point
Compartment syndrome is a time-sensitive surgical emergency. Fasciotomy must be performed within 6–8 hours of symptom onset to prevent irreversible tissue damage. In crush injuries with comminuted fractures, compartment syndrome is a common complication.
Clinical Pearl
The presence of crepitus and severe swelling 6 hours post-injury strongly suggests compartment syndrome. Waiting for imaging or observation risks permanent disability (Volkmann's contracture) and systemic complications (acute kidney injury from myoglobinuria).
High-YieldNEET PG
In crush injuries with comminuted fractures:
Fasciotomy takes priority over fracture fixation
Fracture stabilization can be deferred to a second stage (after soft tissue recovery)
Early fasciotomy prevents the "second hit" of reperfusion injury
Management Sequence in Crush Injury with Compartment Syndrome
Table
Step
Timing
Rationale
Fasciotomy
Immediate (< 6–8 hrs)
Decompress compartments, prevent tissue necrosis
Fluid resuscitation
Concurrent
Prevent rhabdomyolysis-induced AKI
Fracture fixation
Delayed (after soft tissue recovery)
Reduces infection risk, allows wound management
Reconstruction
Later phase
After inflammation subsides
Mnemonic
CRUSH = Compartment syndrome → Recognize early → Urgent fasciotomy → Stable fluids → Health preservation
Why Observation or Casting Fails
Warning
Delaying fasciotomy by even a few hours can result in: