## Ovarian Cancer Prognosis and Treatment in BRCA1 Mutation Carriers **Key Point:** BRCA1/BRCA2 mutations confer a significant survival advantage in epithelial ovarian cancer (EOC) through enhanced platinum sensitivity and eligibility for PARP inhibitor maintenance therapy. ### BRCA Status and Prognosis - **BRCA1/BRCA2-mutant EOC** demonstrates: - Superior platinum sensitivity (homologous recombination deficiency) - Improved progression-free survival (PFS) with platinum-taxol chemotherapy - Improved overall survival (OS) compared to BRCA wild-type tumors - Median OS: 50–60+ months vs. 30–40 months in BRCA wild-type ### Stage IIIC Disease Management - **Optimal cytoreduction** (<1 cm residual) is a major prognostic factor - **Neoadjuvant chemotherapy followed by interval debulking** is now standard for: - Extensive disease (IIIC/IV) - Patients deemed unresectable at initial assessment - Equivalent or superior outcomes to primary debulking in select populations (CHORUS, EORTC trials) ### PARP Inhibitor Maintenance - **BRCA1/BRCA2-mutant, platinum-sensitive EOC:** - Olaparib (SOLO-1 trial): PFS benefit from 13.8 months → not reached; OS benefit emerging - Rucaparib (ARIEL3): PFS improvement in platinum-sensitive recurrence - Recommended as standard maintenance post-chemotherapy in BRCA-mutant patients ### Ascites and Staging - **Ascites alone does NOT define stage IV disease** - Stage IIIC = peritoneal/omental involvement ± ascites - Stage IV = pleural effusion, liver parenchymal involvement, or distant metastases - This patient's ascites is consistent with stage IIIC (peritoneal spread) **High-Yield:** BRCA-mutant EOC + optimal cytoreduction + platinum response = excellent prognosis with PARP inhibitor maintenance. 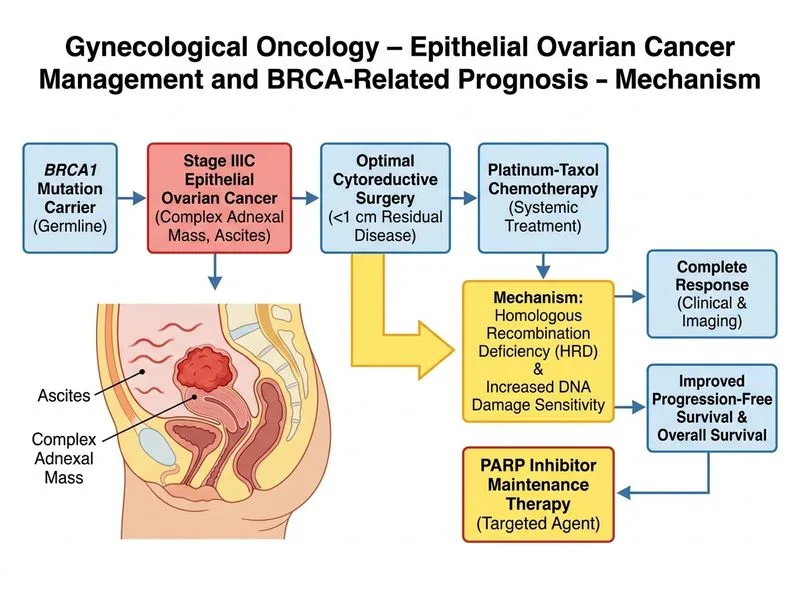
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.