## Clinical Diagnosis: G6PD Deficiency ### Key Clinical Features **Key Point:** The combination of acute hemolytic episodes triggered by oxidative stress (infection, fava beans), bite cells and blister cells on blood smear, and elevated reticulocyte count with indirect hyperbilirubinemia is pathognomonic for G6PD deficiency. ### Diagnostic Hallmarks | Feature | G6PD Deficiency | Hereditary Spherocytosis | AIHA | PNH | |---------|-----------------|-------------------------|------|-----| | **Trigger** | Oxidative stress (drugs, infection, fava beans) | Osmotic stress, infection | Autoimmune | Complement-mediated | | **Blood smear** | Bite cells, blister cells | Spherocytes | Polychromasia, spherocytes | Schistocytes | | **Haptoglobin** | Low | Low | Low | Low | | **DAT (Coombs)** | Negative | Negative | **Positive** | Negative | | **Hemoglobinuria** | Rare | Rare | Possible | **Common** | | **Splenomegaly** | Mild | Moderate | Moderate | Variable | ### Pathophysiology 1. G6PD catalyzes the first step of the pentose phosphate pathway, generating NADPH 2. NADPH maintains reduced glutathione (GSH), which protects RBCs from oxidative damage 3. Deficiency → ↓ GSH → RBC membrane oxidation → hemolysis during oxidative stress 4. Bite cells result from removal of denatured hemoglobin (Heinz bodies) by splenic macrophages **High-Yield:** Bite cells and blister cells are virtually diagnostic of G6PD deficiency and are rarely seen in other hemolytic anemias. ### Confirmatory Testing - **G6PD enzyme assay** (gold standard) — shows reduced enzyme activity - **Heinz body stain** — demonstrates denatured hemoglobin precipitates (especially after oxidative stress) - **Osmotic fragility test** — normal (rules out hereditary spherocytosis) - **DAT (Direct Antiglobulin Test)** — negative (rules out AIHA) **Clinical Pearl:** In acute hemolytic episodes, G6PD levels may appear falsely normal because older RBCs with lower enzyme levels are preferentially lysed, leaving younger cells with higher enzyme activity. Retest 2–3 weeks after resolution of hemolysis for accurate diagnosis. ### Epidemiology & Genetics - X-linked recessive inheritance (predominantly affects males; females are carriers but can have variable expression due to X-inactivation) - Most common enzyme deficiency worldwide (~400 million people) - High prevalence in Mediterranean, African, and Southeast Asian populations - Over 400 genetic variants identified; Class I–III variants cause chronic hemolysis; Class IV–V cause episodic hemolysis only **Mnemonic:** **FADING** — Fava beans, Aspirin, Dapsone, Infections, Nitrofurantoin, Sulfonamides (common triggers of hemolysis in G6PD deficiency). ### Management 1. **Acute episode:** Supportive care, transfusion if Hb <5 g/dL, treat underlying infection 2. **Chronic:** Avoid oxidative triggers, folic acid supplementation 3. **Counseling:** Educate on triggers, genetic inheritance, carrier status in females [cite:Robbins 10e Ch 12] 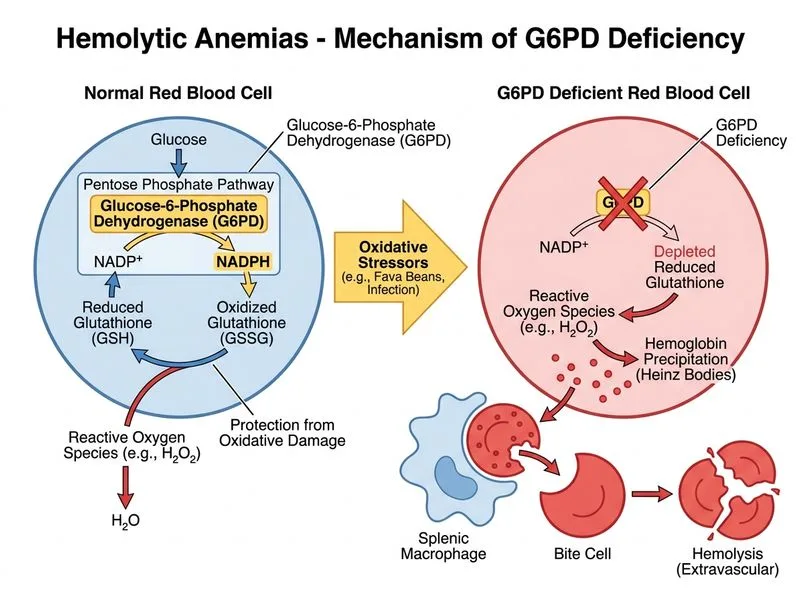
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.