Hepatocellular Carcinoma MCQ — NEET PG Practice Question | NEETPGAI
Hepatocellular Carcinoma
hard
microscope Pathology
A 62-year-old woman with a 15-year history of hepatitis C cirrhosis (Child-Pugh class B) undergoes surveillance imaging and is found to have a 1.5 cm nodule in the left lobe of the liver. Contrast-enhanced CT shows arterial phase hyperenhancement but no washout in the portal venous phase. AFP is 85 ng/mL. Which of the following is the most appropriate next step in management?
A. Perform hepatic resection or transplantation
B. Start sorafenib therapy immediately
C. Repeat imaging in 3–4 months to confirm arterial hyperenhancement and washout
D. Perform liver biopsy to confirm diagnosis of HCC
Explanation
Management of Indeterminate Nodule in Cirrhosis
Diagnostic Uncertainty: The 1–2 cm Nodule Dilemma
Key Point
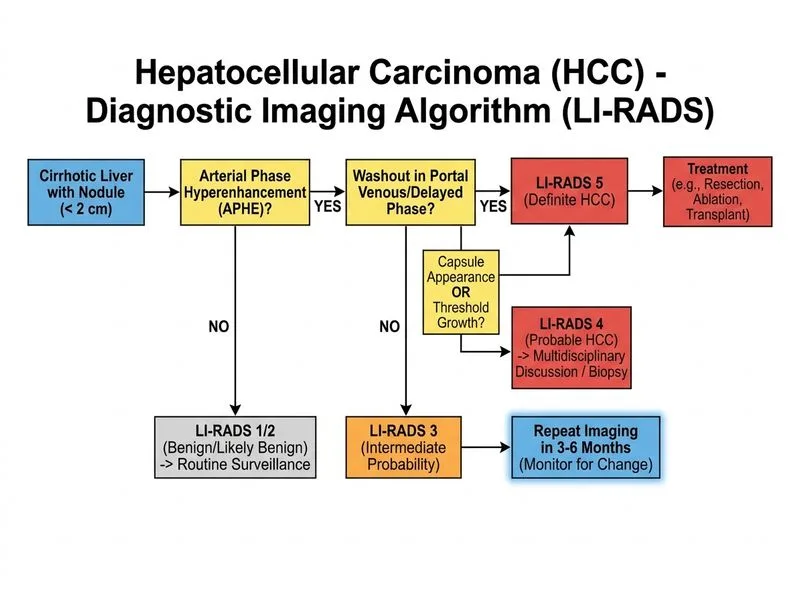
A 1–2 cm nodule with APHE but WITHOUT washout in a cirrhotic liver is indeterminate — it does not meet diagnostic criteria for HCC on a single imaging study. The gold standard approach is repeat imaging in 3–4 months to document both APHE and washout, which would then confirm HCC diagnosis.
AASLD/EASL Diagnostic Algorithm for Nodules in Cirrhosis
Table
Nodule Size
Diagnostic Criteria
>2 cm
APHE + washout on ONE imaging modality (CT/MRI/US) = HCC
1–2 cm
Both APHE + washout on ONE modality, OR APHE on one modality + AFP >400 ng/mL = HCC
<1 cm
Surveillance every 3 months; biopsy if growth
Clinical Pearl
In this case, the nodule shows only APHE without washout, and AFP is 85 ng/mL (not >400). This is not diagnostic for HCC on current imaging. Repeat imaging in 3–4 months is standard practice to:
1.
Confirm persistence of the nodule
2.
Document washout (if present, confirms HCC)
3.
Assess for growth (growth favors malignancy)
Why NOT Biopsy?
High-YieldNEET PG
Biopsy is contraindicated in suspected HCC because:
Risk of tumor seeding along needle tract
Diagnostic criteria (imaging + AFP) are sufficient; biopsy is not required
Biopsy may be falsely negative (sampling error in small nodules)
Bleeding risk in cirrhotic patients with coagulopathy
Why NOT Immediate Treatment?
Sorafenib and resection/transplantation are reserved for confirmed HCC. This nodule is still indeterminate; premature treatment of a benign or dysplastic nodule is inappropriate.