## Hyperkalemia Management in CKD with RAAS Inhibition **Key Point:** In non-emergent hyperkalemia with CKD, RAAS inhibitors should be continued (due to renal and cardiovascular protection) while adding newer potassium binders (patiromer, sodium zirconium cyclosilicate) and dietary counseling. ### Rationale: - **RAAS inhibitors (ACEi/ARB) are cardio-renal protective** in CKD and should not be discontinued for mild-to-moderate hyperkalemia (K 5.5–6.5 mEq/L) without life-threatening ECG changes. - **Newer potassium binders** (patiromer, sodium zirconium cyclosilicate) are superior to sodium polystyrene sulfonate: - Patiromer: non-absorbed, exchanges potassium for calcium in colon; effective and well-tolerated. - Sodium zirconium cyclosilicate: rapid onset, minimal sodium load. - Kayexalate: outdated, associated with colonic necrosis, sorbitol-related complications; no longer first-line. - **Dietary potassium restriction** (target <2 g/day) and monitoring are essential. - **Metabolic acidosis** (HCO₃ 18) may worsen hyperkalemia; correction may help. - **ECG monitoring** is indicated to rule out peaked T waves or QRS prolongation (emergency signs). **Clinical Pearl:** The combination of RAAS inhibitor continuation + newer binder + dietary modification is the evidence-based approach in stable hyperkalemia. **Mnemonic:** **RAAS-K rule** — Retain RAAS inhibitors, Add newer binders, Restrict K⁺, Assess ECG. 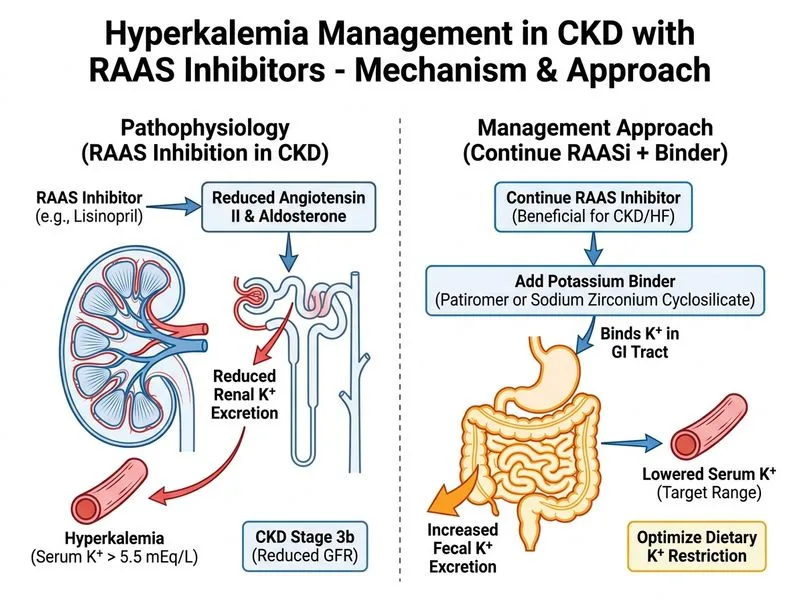
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.