## Diagnosis: Ulcerative Colitis ### Clinical Presentation The patient presents with the classic triad of ulcerative colitis (UC): - **Bloody diarrhea** with mucus - **Continuous abdominal symptoms** over 6 months - **Weight loss** and anemia ### Key Diagnostic Features **Endoscopic Findings:** - **Continuous mucosal inflammation** from rectum to sigmoid (hallmark of UC) - Friability and ulceration confined to the colon - **Normal mucosa proximally** — UC does not skip areas **Histopathology:** - Crypt distortion and chronic inflammation in lamina propria - **Absence of granulomas** — rules out Crohn disease - Inflammation limited to mucosa and submucosa (not transmural) **Laboratory Markers:** - Elevated fecal calprotectin (320 μg/g) indicates active mucosal inflammation - Elevated ESR and anemia reflect chronic inflammation ### Differential Diagnosis Table | Feature | Ulcerative Colitis | Crohn Disease | Infectious Colitis | Ischemic Colitis | | --- | --- | --- | --- | --- | | **Distribution** | Continuous, rectum → proximal | Skip lesions | Variable | Watershed areas | | **Depth** | Mucosa/submucosa | Transmural | Mucosal | Mucosal/submucosal | | **Granulomas** | Absent | Present (50%) | Absent | Absent | | **Rectal involvement** | Always | Variable | Variable | Spared | | **Duration** | Chronic (>4 weeks) | Chronic/relapsing | Acute (days) | Acute/subacute | **Key Point:** The **continuous distribution from rectum without skip lesions** and **absence of granulomas** are pathognomonic for ulcerative colitis. **High-Yield:** UC is confined to the **colon and rectum only**; small bowel involvement is diagnostic of Crohn disease. **Clinical Pearl:** Fecal calprotectin >250 μg/g indicates active IBD; values >400 suggest moderate-to-severe disease. [cite:Robbins 10e Ch 17] 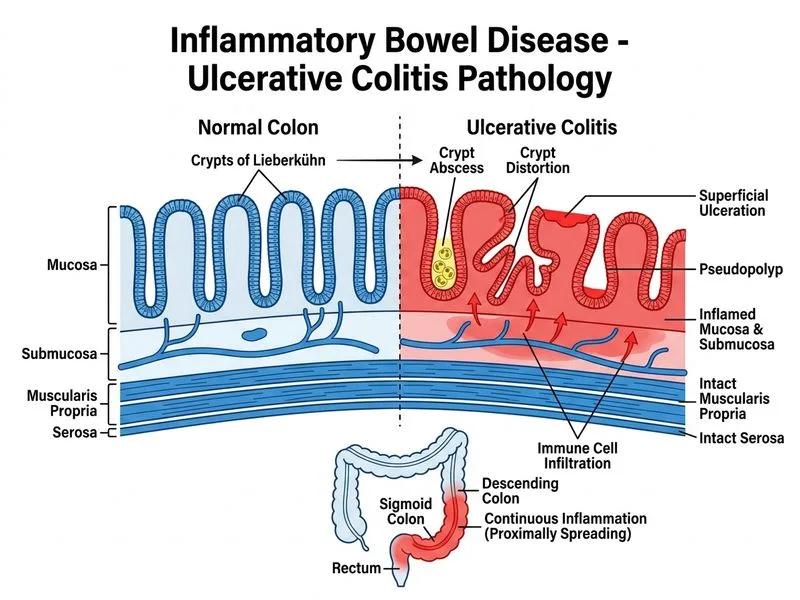
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.