## Diagnosis: Intra-abdominal Abscess ### Clinical Presentation The patient presents with signs of localized infection in the setting of Crohn disease: - **Acute fever** (38.5°C) with elevated WBC and CRP - **Localized abdominal pain** and tenderness in right lower quadrant - **Rebound tenderness and guarding** (peritoneal irritation) - **Known Crohn disease** with poor compliance ### Imaging Findings **CT Abdomen (Gold Standard):** - **6 cm × 5 cm fluid collection** in right iliac fossa — diagnostic of abscess - **Bowel wall thickening** — indicates active Crohn inflammation - **Fistulous tracts** — chronic complication of Crohn disease **Key Point:** The **discrete, localized fluid collection on imaging** is the hallmark of abscess formation. ### Pathophysiology in Crohn Disease ```mermaid flowchart TD A[Crohn Disease with Transmural Inflammation]:::outcome --> B[Bowel Wall Perforation Risk]:::urgent B --> C{Perforation contained?}:::decision C -->|Yes - walled off| D[Intra-abdominal Abscess]:::action C -->|No - free| E[Generalized Peritonitis]:::urgent D --> F[Fever, Leukocytosis, Localized tenderness]:::outcome E --> F2[Acute abdomen, Shock]:::urgent A --> G[Fistula Formation]:::action G --> H[Enterocutaneous or Enteroenteric Fistula]:::outcome ``` ### Complications of Crohn Disease: Comparison Table | Complication | Presentation | Imaging | Management | | --- | --- | --- | --- | | **Abscess** | Localized fever, tenderness, leukocytosis | Fluid collection on CT | Antibiotics + drainage (percutaneous or surgical) | | **Perforation** | Acute severe pain, peritonitis, shock | Free air, no loculation | Emergency surgery | | **Toxic Megacolon** | Severe diarrhea, fever, abdominal distension, systemic toxicity | Colon >6 cm, loss of haustra | Medical management (avoid antidiarrheals) | | **Enterocutaneous Fistula** | Chronic drainage, skin maceration | Contrast studies, fistulography | Nutritional support, antibiotics, surgery if refractory | **High-Yield:** Intra-abdominal abscess is the **most common acute surgical complication of Crohn disease**, occurring in 10–30% of patients. It results from **contained perforation** of a diseased bowel segment. **Clinical Pearl:** The presence of a **discrete, localized fluid collection** on imaging distinguishes abscess from free perforation (which shows free air and generalized peritonitis). **Warning:** Non-compliance with immunosuppressive therapy (azathioprine) increases the risk of disease flares and complications, including abscess formation. [cite:Robbins 10e Ch 17] 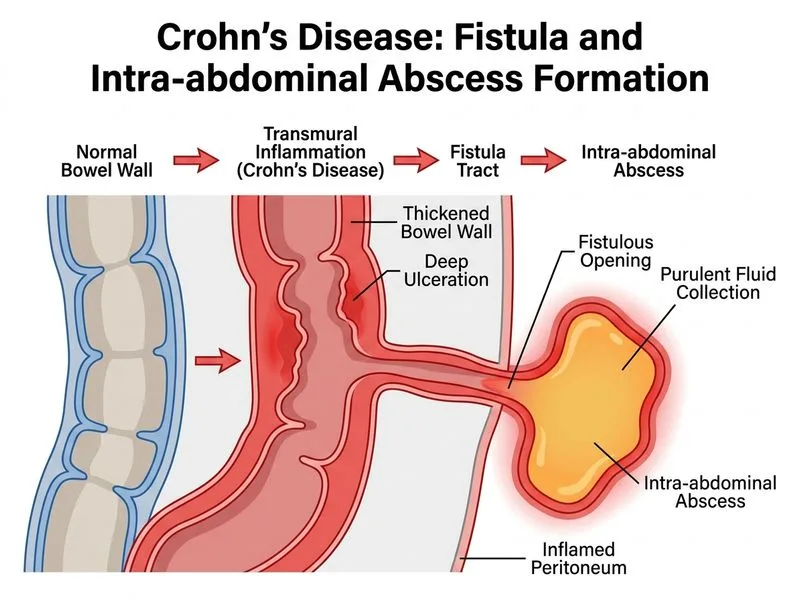
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.