## Awake Fiberoptic Intubation in Predicted Difficult Airway **Key Point:** In patients with severe cervical spine pathology (ankylosing spondylitis, fusion, severe kyphosis) or known/predicted difficult airways, awake fiberoptic intubation (AFOI) is the gold standard approach. ### Rationale for Correct Answer: - **Preserves spontaneous ventilation** and airway reflexes until tube placement is confirmed - **Allows patient cooperation** — the patient can signal distress or positioning problems - **Avoids apnea** — critical in patients where bag-mask ventilation may be impossible - **Dexmedetomidine** (not propofol) is preferred for sedation during AFOI because it maintains respiratory drive and airway reflexes while providing anxiolysis and analgesia - **Topical anesthesia** (lidocaine spray, viscous gel, transtracheal injection) ensures comfort without loss of protective reflexes - This approach has the highest success rate and lowest morbidity in truly difficult airways ### Why AFOI is Superior Here: Ankylosing spondylitis causes progressive cervical fusion and kyphosis, making neck extension impossible. Once induction agents are given, the patient cannot be ventilated (no neck mobility, limited mouth opening), and intubation becomes an emergency. AFOI avoids this trap entirely. **Clinical Pearl:** The rule is: *predict difficult airway → awake approach*. Never induce a patient with a predicted difficult airway unless you are 100% certain of immediate rescue options. ## Comparison Table | Approach | Ankylosing Spondylitis | Preserves Reflexes | Risk of Apnea | Operator Skill | |----------|------------------------|-------------------|---------------|----------------| | Awake FOI | ✓ Ideal | ✓ Yes | ✓ No | High | | RSI + MILS | ✗ Poor | ✗ No | ✗ High | Moderate | | Blind nasal | ✗ Risky | ✗ No | ✗ High | Moderate | | Cricothyrotomy | Emergency only | N/A | N/A | High | **High-Yield:** AFOI is indicated for: predicted difficult airway, cervical spine instability/pathology, severe TMJ dysfunction, ankylosing spondylitis, epiglottitis, angioedema, and awake extubation in high-risk patients. 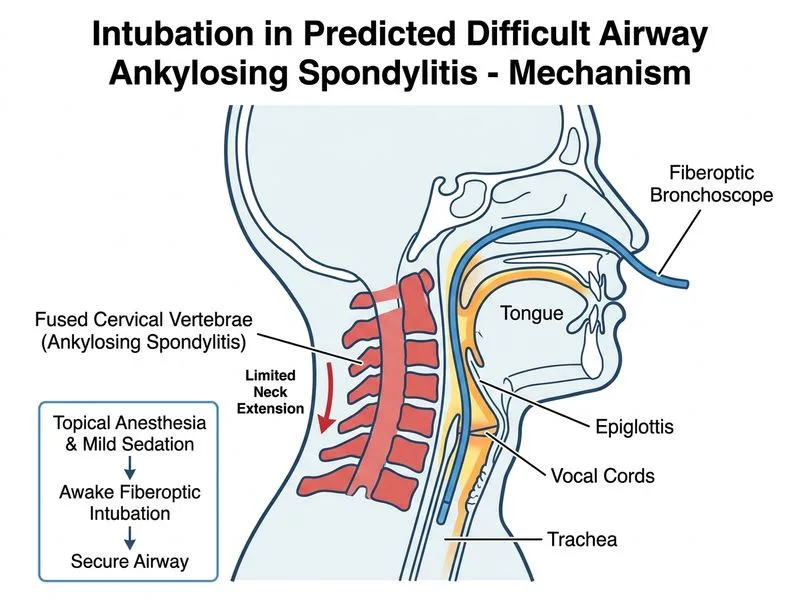
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.