## Diagnosis: Iron Deficiency Anemia Secondary to Chronic Menorrhagia ### Clinical Presentation The patient presents with a classic triad of iron deficiency anemia: - **Symptoms**: Progressive fatigue, dyspnea on exertion, palpitations - **Source of blood loss**: Heavy menstrual bleeding (menorrhagia) for 2 years — the most common cause of iron deficiency in non-pregnant women - **Physical signs**: Pallor, conjunctival pallor, systolic flow murmur (high-output cardiac state) ### Laboratory Findings — The Diagnostic Hallmark | Parameter | Finding | Interpretation | |-----------|---------|----------------| | Hemoglobin | 7.2 g/dL | Moderate anemia | | MCV | 58 fL | Microcytic (< 80 fL) | | MCH | 19 pg | Hypochromic (< 27 pg) | | Serum ferritin | 12 ng/mL | **Depleted iron stores** (normal > 30 ng/mL) | | Serum iron | 35 µg/dL | Low (normal 60–170 µg/dL) | | TIBC | 420 µg/dL | **Elevated** (normal 250–425 µg/dL) — reflects increased iron demand | | Transferrin saturation | 8% | **Very low** (normal 20–50%) | | Peripheral smear | Microcytic hypochromic RBCs, target cells | Consistent with iron deficiency | **Key Point:** The combination of **low serum ferritin + low serum iron + elevated TIBC + low transferrin saturation** is pathognomonic for iron deficiency anemia. Ferritin is the most sensitive marker of depleted iron stores. ### Pathophysiology 1. Chronic menorrhagia → ongoing blood loss 2. Iron stores depleted (ferritin ↓) 3. Serum iron falls, TIBC rises (compensatory increase in transferrin synthesis) 4. Insufficient iron for hemoglobin synthesis → microcytic, hypochromic RBCs 5. Reduced oxygen-carrying capacity → high-output state (tachycardia, flow murmur) **Clinical Pearl:** The systolic flow murmur at the apex is a sign of high-output cardiac compensation in severe anemia, not structural mitral valve disease. ### Peripheral Blood Smear Findings in Iron Deficiency - Microcytic RBCs (small cell size) - Hypochromic RBCs (increased central pallor) - Target cells (codocytes) — due to reduced hemoglobin content - Occasional pencil cells (elliptocytes) - Anisocytosis (variation in RBC size) **High-Yield:** Iron deficiency anemia is the most common cause of microcytic anemia worldwide. In women of reproductive age, menorrhagia is the leading cause; in men and postmenopausal women, GI blood loss must be excluded. **Mnemonic — Causes of Iron Deficiency:** **BLOOD** - **B**leeding (GI, GYN, other) - **L**ow intake (dietary, malabsorption) - **O**ther losses (hemolysis — rare in pure IDA) - **O**bstetric (pregnancy, lactation) - **D**ietary deficiency (rare in developed countries) ### Why This Is Iron Deficiency and Not Other Microcytic Anemias - **vs. Thalassemia trait**: Ferritin is normal or elevated in thalassemia (iron overload from hemolysis); TIBC is normal. Here, ferritin is low and TIBC is high — opposite pattern. - **vs. Anemia of chronic disease**: Would have normal or elevated ferritin and normal or low TIBC. This patient's ferritin is depleted. - **vs. Sideroblastic anemia**: Serum iron and ferritin are typically elevated (iron accumulation); TIBC is low. This patient has the opposite. **Tip:** Always measure serum ferritin first in suspected iron deficiency — it is the most cost-effective and sensitive test for iron store depletion. 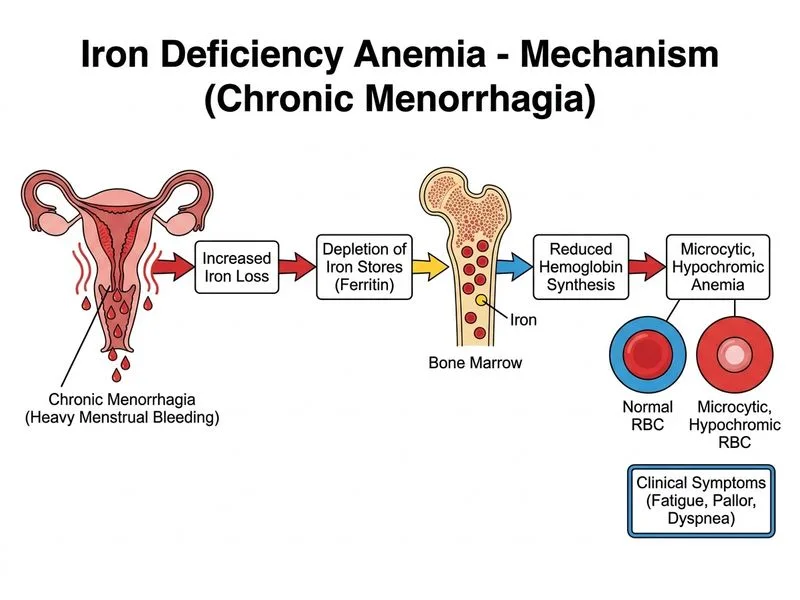
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.