## Clinical Scenario Analysis This patient presents with **acute ischemic stroke in the setting of atrial fibrillation, 5 hours after symptom onset**. The key clinical decision is whether she is a candidate for reperfusion therapy and what modality is most appropriate. ## Time Window Analysis **High-Yield:** The patient is **BEYOND the 3-hour IV thrombolysis window** (5 hours elapsed) and at the **upper limit of the extended 4.5-hour window** (only if specific criteria are met: age <80, NIHSS ≤25, no diabetes history, no prior stroke). **Key Point:** At 5 hours, **mechanical thrombectomy (MT) becomes the preferred reperfusion strategy** if large vessel occlusion (LVO) is present, as it has superior outcomes to delayed IV thrombolysis in the extended window. ## Why CTA + Thrombectomy? **Clinical Pearl:** The **DAWN and DEFUSE-3 trials** demonstrated that mechanical thrombectomy is effective up to **24 hours** in selected patients with LVO and favorable imaging (penumbra-core mismatch). At 5 hours, she is well within the thrombectomy window. **Mnemonic: LVO THROMBECTOMY WINDOW = Up to 24 hours with favorable imaging (penumbra present)** ## Why NOT IV Alteplase? 1. **5 hours is beyond the standard 3-hour window** — benefit diminishes significantly 2. **Extended window (3–4.5 hrs) has strict exclusion criteria** — this patient's exact eligibility is unclear from the stem 3. **If LVO is present, MT is superior** to IV thrombolysis alone in the extended window ## Role of Anticoagulation **Warning:** Acute anticoagulation (heparin) in acute ischemic stroke is **NOT standard therapy** and may increase hemorrhagic transformation risk. Anticoagulation is reserved for specific indications (e.g., cardioembolic stroke with high recurrence risk) and is typically started **after ruling out hemorrhage and after initial reperfusion attempts**. ## Atrial Fibrillation Management Long-term anticoagulation (warfarin, DOACs) is essential for secondary stroke prevention in AF, but this is initiated **after acute phase management**, not immediately. ```mermaid flowchart TD A["Acute Ischemic Stroke"]:::outcome --> B{"Time from onset?"}:::decision B -->|"< 3 hours"| C["IV Alteplase"]:::action B -->|"3-4.5 hours"| D{"Strict criteria met?"}:::decision B -->|"4.5-24 hours"| E{"LVO on CTA?"}:::decision D -->|"Yes"| C D -->|"No"| E E -->|"Yes"| F["Mechanical Thrombectomy"]:::action E -->|"No"| G["Medical Management + Anticoagulation"]:::action C --> H["Reperfusion achieved"]:::outcome F --> H G --> I["Prevent recurrence"]:::outcome ``` [cite:Harrison 21e Ch 372] 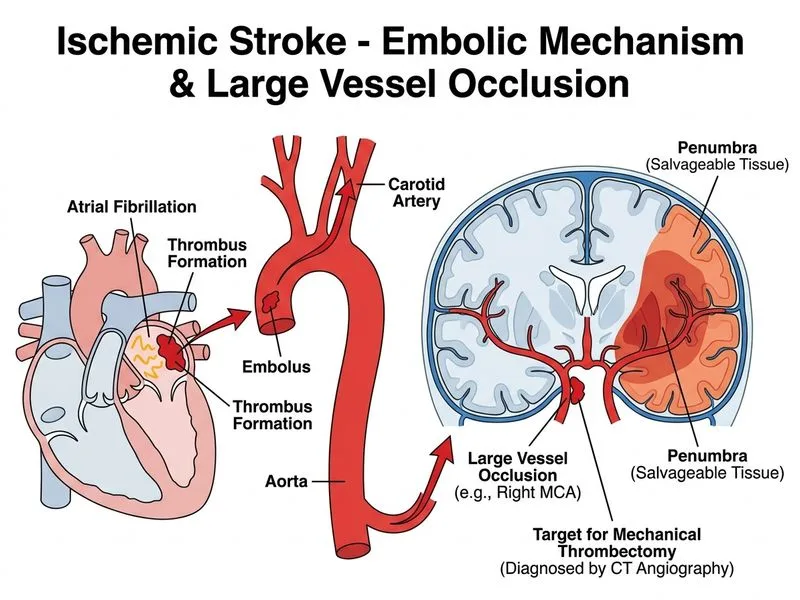
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.