## Clinical Scenario Analysis This patient presents **beyond the 4.5-hour thrombolytic window** (last known well 18 hours ago) with acute ischemic stroke in the MCA territory, likely cardioembolic given her atrial fibrillation. The key question is: what is the **most appropriate acute management**? ## Why Thrombolysis Is Contraindicated (Option C) **Key Point:** IV alteplase is only indicated within **4.5 hours** of symptom onset (or last known well). At 18 hours, the risk of hemorrhagic transformation far exceeds any reperfusion benefit. This option is clearly incorrect. ## Why Mechanical Thrombectomy Is Not the Answer Here (Option B) Mechanical thrombectomy can be considered up to **24 hours** in selected patients with large vessel occlusion (LVO) and favorable perfusion imaging (DAWN/DEFUSE-3 criteria). However, the stem does **not** mention LVO on imaging, no CT/MR angiography findings are provided, and the question asks for the **most appropriate acute management** — not a conditional intervention. Without confirmed LVO, thrombectomy is not the default answer. ## Why Early Anticoagulation Is NOT Recommended Acutely (Option D) **High-Yield:** Current AHA/ASA 2019 and ESO 2021 guidelines do **not** recommend urgent anticoagulation (UFH or LMWH) in the acute phase of ischemic stroke, even in cardioembolic stroke due to AF. The risk of hemorrhagic transformation of a large MCA territory infarct outweighs the benefit of early anticoagulation. The standard recommendation is to **delay anticoagulation** for at least 48 hours to 2 weeks depending on infarct size, and to use **aspirin** in the interim. > *"Urgent anticoagulation with the goal of preventing early recurrent stroke, halting neurological worsening, or improving outcomes after acute ischemic stroke is not recommended."* — AHA/ASA Stroke Guidelines 2019 (Class III, Level of Evidence A) ## Why Aspirin Monotherapy Is Correct (Option A) **Clinical Pearl:** In acute ischemic stroke beyond the thrombolytic window, **aspirin 300 mg** (loading dose) is the cornerstone of acute antiplatelet therapy. Dual antiplatelet therapy (aspirin + clopidogrel) is recommended for **minor stroke or high-risk TIA** (POINT/CHANCE trials), but for a major MCA territory stroke, aspirin monotherapy is the standard acute treatment. The stem does not describe a minor stroke, so aspirin 300 mg alone is the most appropriate answer among the options given. ## Summary Table | Option | Verdict | Reason | |--------|---------|--------| | **A: Aspirin 300 mg** | ✅ Correct | Standard acute management beyond thrombolytic window | | B: Mechanical thrombectomy | ❌ Incorrect | No LVO confirmed; specific imaging criteria not met | | C: IV alteplase | ❌ Incorrect | Outside 4.5-hour window | | D: Aspirin + UFH | ❌ Incorrect | Early anticoagulation not recommended acutely in large MCA infarct (hemorrhage risk) | **High-Yield:** Per AHA/ASA 2019 guidelines, aspirin 325 mg within 24–48 hours of stroke onset is a Class I, Level A recommendation. Anticoagulation for AF-related stroke should be initiated **after** the acute phase (typically 4–14 days depending on infarct size), not immediately. *(Reference: AHA/ASA Guidelines for the Early Management of Patients with Acute Ischemic Stroke, Stroke 2019; Harrison's Principles of Internal Medicine, 21st ed., Chapter on Cerebrovascular Disease)* 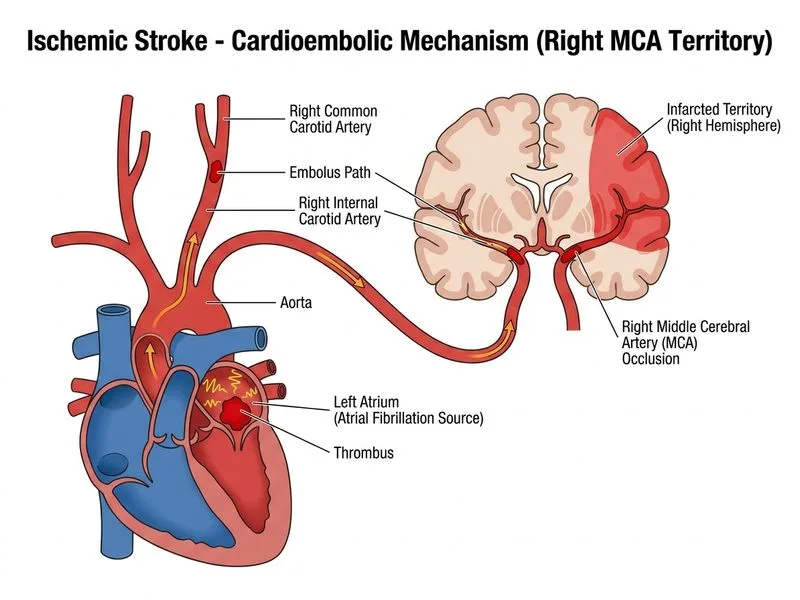
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.