## Clinical Assessment This patient presents with acute ischemic stroke within the thrombolytic window (2 hours from onset). The non-contrast CT excludes hemorrhage, which is the critical prerequisite for thrombolysis eligibility. ### Key Point: **Time is brain.** Intravenous thrombolysis (IV-tPA/alteplase) is the standard of care for acute ischemic stroke within 4.5 hours of symptom onset, provided there are no contraindications (hemorrhage, recent surgery, anticoagulation, severe thrombocytopenia). ### High-Yield: The dose of alteplase for acute ischemic stroke is **0.9 mg/kg (maximum 90 mg)**, with 10% given as a bolus over 1 minute and the remainder over 60 minutes. This patient has no absolute contraindications: his blood glucose (186 mg/dL) is acceptable, and the time window is within 3 hours. ### Clinical Pearl: In acute stroke, **do not delay thrombolysis to obtain additional imaging** (CT angiography, MRI) unless there is clinical suspicion of hemorrhage or contraindication. The non-contrast CT has ruled out hemorrhage; proceed with fibrinolysis. ### Mnemonic: CONTRAINDICATIONS to IV-tPA in Stroke - **C**urrent anticoagulation (INR >1.7) - **O**ngoing seizure - **N**ew intracranial pathology (hemorrhage, mass) - **T**raumatic LP <7 days, intracranial surgery <3 months - **R**ecent MI or stroke (<3 months) - **A**ctive bleeding, thrombocytopenia (<100,000) - **I**nfective endocarditis - **N**eed for urgent surgery - **D**issecting aorta - **I**ntracranial hemorrhage on imaging - **C**oagulopathy (PT/INR prolonged) - **A**spirin allergy (relative) - **T**ransient symptoms resolving (relative) - **I**ncreased intracranial pressure - **O**ral anticoagulation (relative if INR <1.7) - **N**ew stroke on anticoagulation (relative) - **S**evere hypertension unresponsive to treatment (SBP >185, DBP >110) [cite:Harrison 21e Ch 386] 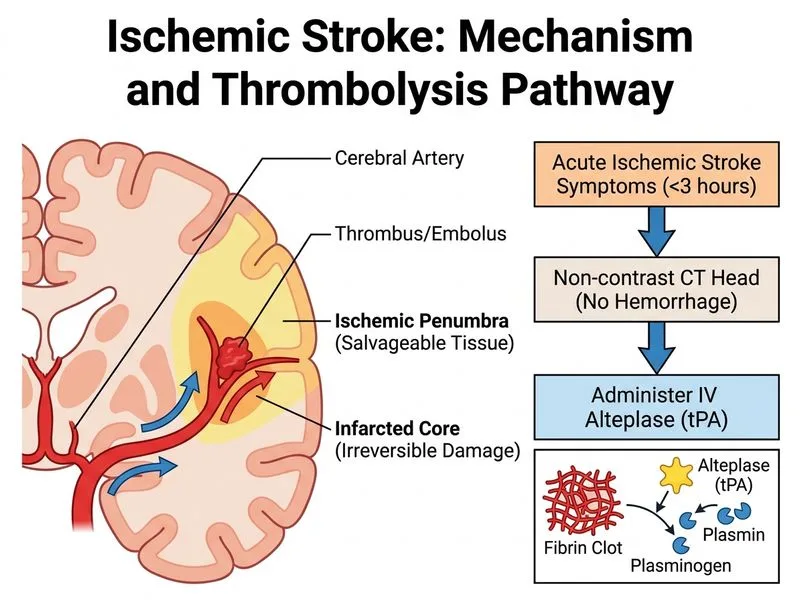
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.