## Clinical Context This patient has acute ischemic stroke in the setting of atrial fibrillation, presenting beyond the IV-tPA window (6 hours from wake-up time = unknown actual onset). The MRI DWI confirms acute ischemia in the MCA territory, suggesting a proximal arterial occlusion. ### Key Point: **Mechanical thrombectomy is indicated for acute ischemic stroke with large vessel occlusion (LVO) within 24 hours of symptom onset (or last known well time), provided there is salvageable brain tissue.** This patient is within the extended thrombectomy window and has imaging evidence of acute stroke. ### High-Yield: The DAWN and DEFUSE-3 trials established that thrombectomy is beneficial up to 24 hours after last known well time in carefully selected patients with: - Large vessel occlusion (ICA, MCA M1, basilar artery) - Salvageable tissue (mismatch between infarct core and penumbra on perfusion imaging or clinical/imaging discordance) - NIHSS ≥6 (this patient has aphasia + hemiparesis, suggesting NIHSS >6) ### Clinical Pearl: In wake-up strokes, the time of symptom onset is unknown; the "last known well" time (when patient fell asleep) is used. This patient qualifies for the extended thrombectomy window. **CTA is mandatory to confirm LVO before proceeding to thrombectomy.** ### Mnemonic: THROMBECTOMY CRITERIA (DAWN/DEFUSE-3) - **T**ime: <24 hours from last known well - **H**yperdensity or occlusion on imaging (CTA/MRA) - **R**escue-worthy: NIHSS ≥6 - **O**cclusion: ICA, M1-MCA, basilar artery - **M**ismatch: infarct core <70 mL, perfusion deficit >15 mL - **B**rain tissue salvageable (penumbra present) - **E**ligible: no contraindications (severe coagulopathy, recent surgery) - **C**TA/MRA confirmation of LVO - **T**ransfer to thrombectomy-capable center if needed - **O**pen artery = goal - **M**ost effective within 6 hours but beneficial to 24 hours - **Y**ield: 50% achieve mTICI 2b-3 (good reperfusion) [cite:Harrison 21e Ch 386; NEJM 2018 DAWN Trial] 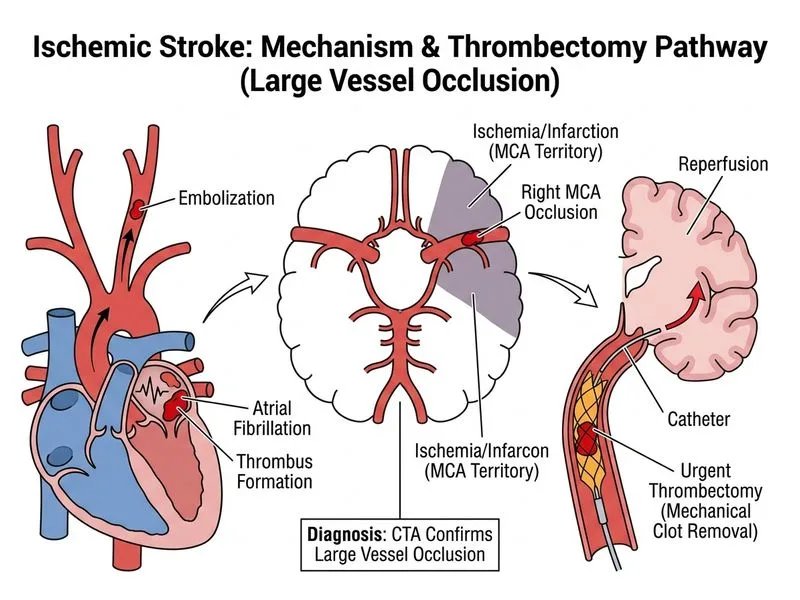
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.