Lung Cancer — Non-Small Cell MCQ — NEET PG Practice Question | NEETPGAI
Lung Cancer — Non-Small Cell
hard
microscope Pathology
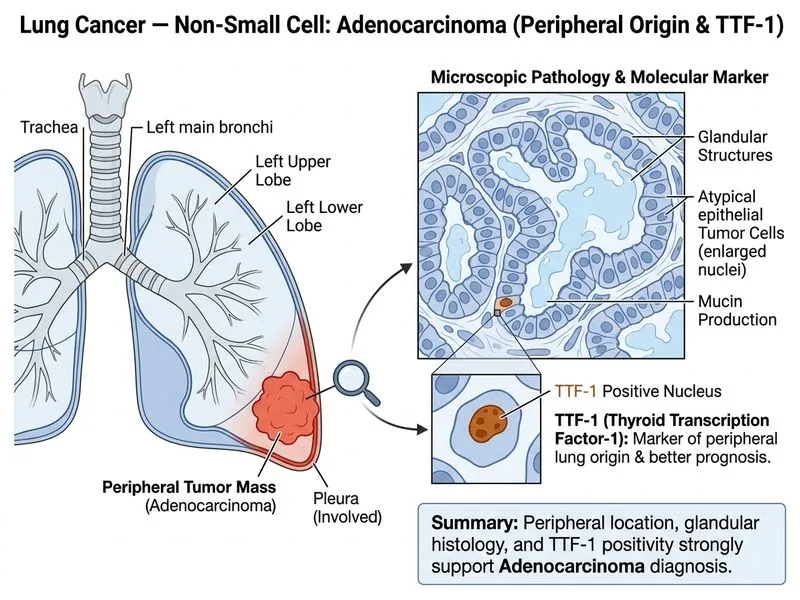
A 62-year-old woman with no smoking history presents with progressive dyspnoea and chest pain. Chest X-ray shows a 5 cm mass in the left lower lobe with pleural involvement. CT chest confirms T4N2M0 disease. Bronchoscopy shows no endobronchial lesion. Biopsy reveals a well-differentiated tumour with mucin-producing glandular structures and absence of keratinization. Immunohistochemistry is positive for TTF-1 and CK7. What is the most likely histological type and what is the significance of TTF-1 positivity?
A. Squamous cell carcinoma; TTF-1 indicates central airway involvement
B. Adenosquamous carcinoma; TTF-1 indicates mixed histology
C. Large cell carcinoma; TTF-1 indicates neuroendocrine differentiation
D. Adenocarcinoma; TTF-1 indicates peripheral lung origin and better prognosis
Explanation
Diagnosis: Adenocarcinoma with TTF-1 Positivity
Key Point
Adenocarcinoma is characterized by mucin-producing glandular structures and is the most common lung cancer in non-smokers. TTF-1 (Thyroid Transcription Factor-1) is a lineage-specific marker of lung and thyroid origin.
Histological Features of Adenocarcinoma
Table
Feature
Adenocarcinoma
Squamous Cell
Large Cell
Glandular structures
Present (hallmark)
Absent
Absent
Mucin production
Present
Absent
Absent
Keratinization
Absent
Present
Absent
Smoking association
Weak (30%)
Very strong (90%)
Strong
Location
Peripheral (distal airways)
Central (proximal airways)
Variable
TTF-1 positivity
80–90%
10–20%
Variable
Immunohistochemical Profile
High-YieldNEET PG
Adenocarcinoma shows:
TTF-1 positive (80–90% of cases) — indicates pulmonary origin
Confirms pulmonary origin — rules out metastatic adenocarcinoma from stomach, colon, or pancreas
2.
Prognostic marker — TTF-1+ adenocarcinomas have slightly better prognosis than TTF-1– adenocarcinomas
3.
Therapeutic relevance — helps guide molecular testing for EGFR mutations and ALK rearrangements (more common in TTF-1+ adenocarcinomas)
4.
Peripheral location — TTF-1+ adenocarcinomas typically arise from peripheral airways (Clara cells, type II pneumocytes)
Why Peripheral Location Matters
Warning
Adenocarcinoma arises from distal airways and can present as a peripheral nodule without endobronchial involvement — this patient had no endobronchial lesion on bronchoscopy, which is consistent with adenocarcinoma, NOT squamous cell carcinoma (which typically shows central/endobronchial involvement).
Staging & Prognosis Context
This patient has T4N2M0 disease (stage IIIB) with pleural involvement, indicating locally advanced but potentially resectable disease. TTF-1 positivity supports molecular profiling for targeted therapy (EGFR inhibitors, ALK inhibitors).
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.