## Paraneoplastic Syndrome in SCLC **Key Point:** The clinical and laboratory findings are diagnostic of **Syndrome of Inappropriate Antidiuretic Hormone (SIADH)** secretion: hyponatremia with low serum osmolality, inappropriately elevated urine osmolality, and high urine sodium in the setting of SCLC. ### Laboratory Criteria for SIADH | Parameter | Expected Value | This Patient | |-----------|----------------|---------------| | Serum sodium | 135–145 mEq/L | 118 (↓) | | Serum osmolality | 280–295 mOsm/kg | 245 (↓) | | Urine osmolality | <100 mOsm/kg (in hyponatremia) | 580 (↑) | | Urine sodium | <20 mEq/L (in hyponatremia) | 85 (↑) | | TSH, cortisol | Normal | Normal | **High-Yield:** SIADH is the **most common paraneoplastic endocrine syndrome in SCLC**, occurring in 10–15% of cases. The malignant cells produce and secrete ADH (vasopressin), leading to water retention and dilutional hyponatremia. ### Paraneoplastic Syndromes in SCLC: Comparative Table | Syndrome | Mechanism | Frequency | Clinical Features | |----------|-----------|-----------|-------------------| | **SIADH** | ADH secretion by tumor cells | 10–15% | Hyponatremia, confusion, seizures, weakness | | **Cushing syndrome** | Ectopic ACTH secretion | 5% | Hypokalemia, metabolic alkalosis, hypertension, hyperglycemia | | **Hypercalcemia** | PTHrP or calcitriol secretion | 5% | Polyuria, polydipsia, confusion, constipation | | **LEMS** | Anti-P/Q-type calcium channel antibodies | 3% | Proximal muscle weakness, autonomic dysfunction, areflexia | **Clinical Pearl:** In SIADH, the kidneys continue to excrete sodium despite hyponatremia (urine sodium >20 mEq/L), distinguishing it from hyponatremia due to volume depletion or cirrhosis, where urine sodium is low. ### Mechanism of SIADH in SCLC ```mermaid flowchart TD A[SCLC cells]:::outcome --> B[Produce and release ADH]:::action B --> C[Increased water reabsorption in collecting duct]:::action C --> D[Plasma volume expansion]:::action D --> E[Dilutional hyponatremia]:::outcome D --> F[Suppression of renin-angiotensin-aldosterone]:::action F --> G[Increased urinary sodium excretion]:::action G --> H[Urine osmolality remains high despite low serum osmolality]:::outcome ``` **Warning:** Do not confuse SIADH with other causes of hyponatremia. In this case, the inappropriately high urine osmolality (580 mOsm/kg) in the setting of low serum osmolality (245 mOsm/kg) is pathognomonic for SIADH — the kidneys are unable to suppress ADH despite plasma hypoosmolality. ### Management of SIADH in SCLC 1. **Acute symptomatic hyponatremia:** Hypertonic saline (3% NaCl) with careful sodium correction (6–8 mEq/L per 24 hours to avoid osmotic demyelination) 2. **Chronic SIADH:** Fluid restriction (500–1000 mL/day) 3. **Definitive treatment:** Chemotherapy for SCLC (platinum-etoposide regimen often resolves SIADH as tumor burden decreases) 4. **Refractory cases:** Vaptans (vasopressin antagonists) such as tolvaptan [cite:Harrison 21e Ch 97; Robbins 10e Ch 15] 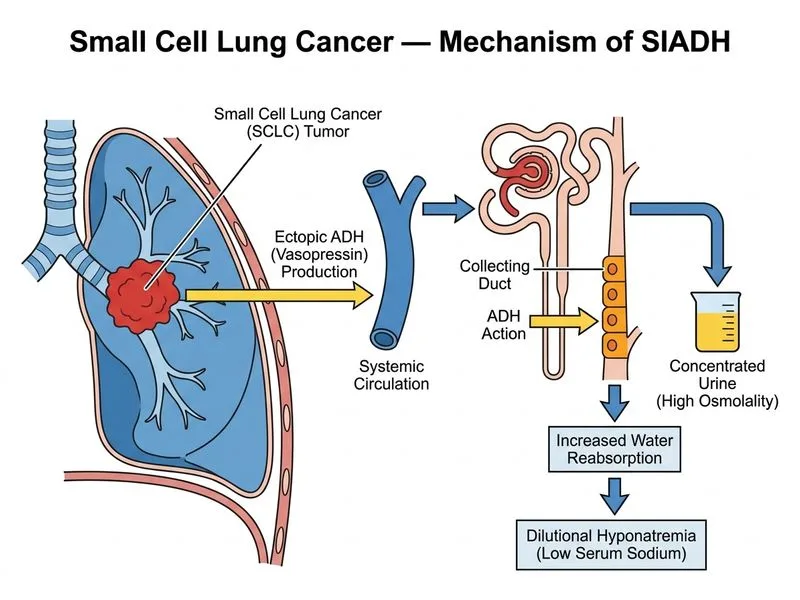
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.