## Diagnosis: Nodular Sclerosis Hodgkin Lymphoma ### Histopathologic Features **Key Point:** The description of large multinucleated cells with prominent eosinophilic nucleoli surrounded by a rich inflammatory background is pathognomonic for Reed-Sternberg (RS) cells and Hodgkin-variant RS cells, the hallmark of Hodgkin lymphoma (HL). ### Immunophenotype **High-Yield:** The immunophenotype CD30+, CD15+, CD45−, CD20− is diagnostic of Hodgkin lymphoma. The neoplastic cells are: - CD30+ (activation antigen, present on RS cells) - CD15+ (present in ~75% of classical HL) - CD45− (negative, distinguishes from reactive lymphocytes) - CD20− (negative, distinguishes from B-cell lymphomas) ### Why Nodular Sclerosis? **Clinical Pearl:** Nodular sclerosis is the most common subtype of classical Hodgkin lymphoma (60–70% of cases), typically presents with mediastinal and supraclavicular/cervical involvement in young adults, and shows nodular fibrosis with lacunar cells (RS cell variants in formalin-fixed tissue). ### Pathologic Subtypes of Classical Hodgkin Lymphoma | Subtype | Frequency | Key Features | Prognosis | |---------|-----------|--------------|----------| | Nodular sclerosis | 60–70% | Nodular fibrosis, lacunar cells, mediastinal involvement | Favorable | | Mixed cellularity | 15–25% | Numerous RS cells, mixed inflammatory background | Intermediate | | Lymphocyte-rich | 5% | Few RS cells, abundant small lymphocytes | Favorable | | Lymphocyte-depleted | <5% | Numerous RS cells, sparse lymphocytes | Unfavorable | **Mnemonic:** **NMLLD** = Nodular sclerosis, Mixed cellularity, Lymphocyte-rich, Lymphocyte-depleted (in order of decreasing frequency). ### Clinical Presentation **Key Point:** Young adults (15–35 years), painless lymphadenopathy (often cervical/mediastinal), B symptoms (fever, night sweats, weight loss) in ~30% of cases at diagnosis. 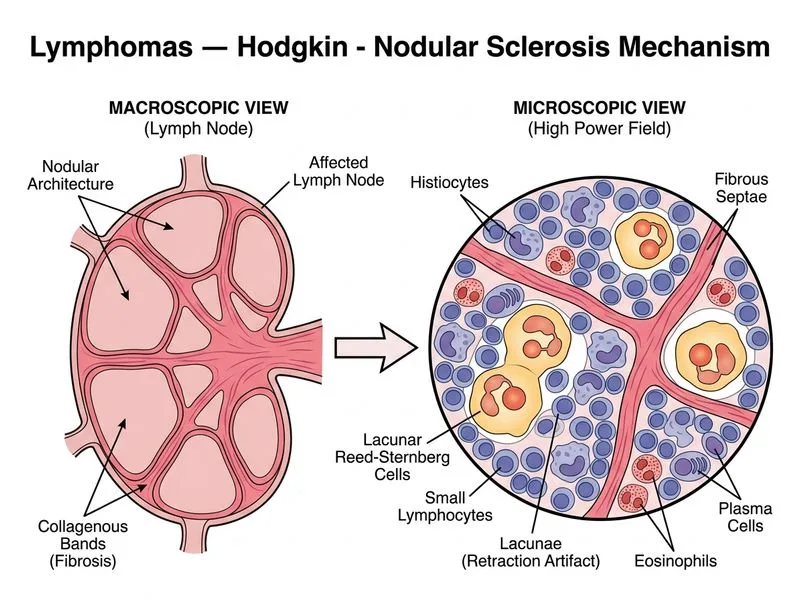
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.